Lymphoma
| Lymphoma | |
|---|---|
 | |
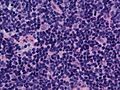
Follicular lymphoma replacing a lymph node | |
| Specialty | Hematology and oncology |
| Symptoms | Enlarged lymph nodes, fever, sweats, unintended weight loss, itching, feeling tired[1][2] |
| Risk factors | Epstein–Barr virus, autoimmune diseases, HIV/AIDS, tobacco smoking[2][3] |
| Diagnostic method | Lymph node biopsy[1][2] |
| Treatment | Chemotherapy, radiation therapy, targeted therapy, surgery[1][2] |
| Prognosis | Average five year survival 85% (USA)[4] |
| Frequency | 4.9 million (2015)[5] |
| Deaths | 204,700 (2015)[6] |
Lymphoma is a group of blood cancers that develop from lymphocytes (a type of white blood cell).[7] The name often refers to just the cancerous versions rather than all such tumors.[7] Signs and symptoms may include enlarged lymph nodes, fever, drenching sweats, unintended weight loss, itching, and constantly feeling tired.[1][2] The enlarged lymph nodes are usually painless.[1] The sweats are most common at night.[1][2]
There are many subtypes of lymphomas.[8] The two main categories of lymphomas are Hodgkin's lymphomas (HL) and the non-Hodgkin lymphomas (NHL).[9] The World Health Organization (WHO) includes two other categories as types of lymphoma: multiple myeloma and immunoproliferative diseases.[10] About 90% of lymphomas are non-Hodgkin lymphomas.[9][11] Lymphomas and leukemias are a part of the broader group of tumors of the hematopoietic and lymphoid tissues.[12]
Risk factors for Hodgkin lymphoma include infection with Epstein–Barr virus and a history of the disease in the family.[1] Risk factors for common types of non-Hodgkin lymphomas include autoimmune diseases, HIV/AIDS, infection with human T-lymphotropic virus, immunosuppressant medications, and some pesticides.[2][13] Eating large amounts of red meat and tobacco smoking may also increase the risk.[3][14][15] Diagnosis, if enlarged lymph nodes are present, is usually by lymph node biopsy.[1][2] Blood, urine, and bone marrow testing may also be useful in the diagnosis.[2]Medical imaging may then be done to determine if and where the cancer has spread.[1][2] Lymphoma most often spreads to the lungs, liver, and brain.[1][2]
Treatment may involve one or more of the following: chemotherapy, radiation therapy, targeted therapy, and surgery.[1][2] In some non-Hodgkin lymphomas, an increased amount of protein produced by the lymphoma cells causes the blood to become so thick that plasmapheresis is performed to remove the protein.[2]Watchful waiting may be appropriate for certain types.[2] The outcome depends on the subtype with some being curable and treatment prolonging survival in most.[9] The five-year survival rate in the United States for all Hodgkin lymphoma subtypes is 85%,[4] while that for non-Hodgkin lymphomas is 69%.[16] Worldwide, lymphomas developed in 566,000 people in 2012 and caused 305,000 deaths.[10] They make up 3–4% of all cancers, making them as a group the seventh-most common form.[10][17] In children, they are the third-most common cancer.[18] They occur more often in the developed world than the developing world.[10].mw-parser-output .toclimit-2 .toclevel-1 ul,.mw-parser-output .toclimit-3 .toclevel-2 ul,.mw-parser-output .toclimit-4 .toclevel-3 ul,.mw-parser-output .toclimit-5 .toclevel-4 ul,.mw-parser-output .toclimit-6 .toclevel-5 ul,.mw-parser-output .toclimit-7 .toclevel-6 ul{display:none}
Contents
1 Signs and symptoms
2 Diagnosis
2.1 Classification
2.1.1 Hodgkin lymphoma
2.1.2 Non-Hodgkin lymphomas
2.1.3 Epstein-Barr virus-associated lymphoproliferative diseases
2.1.4 WHO classification
2.1.5 Previous classifications
2.2 Staging
2.3 Differential diagnosis
3 Treatment
3.1 Low-grade
3.2 High-grade
3.2.1 Hodgkin lymphoma
3.3 Palliative care
4 Prognosis
5 Epidemiology
6 History
7 Research
8 Other animals
9 References
10 External links
Signs and symptoms

The lymph nodes where lymphoma most commonly develops

Lymphoma and lymphatic system
Lymphoma may present with certain nonspecific symptoms; if the symptoms are persistent, an evaluation to determine their cause, including possible lymphoma, should be undertaken.
Lymphadenopathy[19][20] or swelling of lymph nodes, is the primary presentation in lymphoma.
B symptoms (systemic symptoms) – can be associated with both Hodgkin lymphoma and non-Hodgkin lymphoma. They consist of:
Fever[19][20]
Night sweats[19][20]
Weight loss[19][20]
- Other symptoms:
Loss of appetite or anorexia[20]
Fatigue[19][20]
Respiratory distress or dyspnea[20]
Itching[19][20]
Diagnosis

Lymphoma may appear as peritoneal lymphomatosis, as can be seen on CT scan. Image depicts non-Hodgkin lymphoma in a 17 year old HIV positive patient. A. Irregular homogenously enhancing wall thickening involving the ileocaecal region with aneurysmal dilatation of involved segments (curved arrow). B. Hepatosplenomegaly with hepatic metastasis (white arrows).[21]
Lymphoma is definitively diagnosed by a lymph node biopsy, meaning a partial or total excision of a lymph node examined under the microscope.[22] This examination reveals histopathological features that may indicate lymphoma. After lymphoma is diagnosed, a variety of tests may be carried out to look for specific features characteristic of different types of lymphoma. These include:
- Immunophenotyping
- Flow cytometry
Fluorescence in situ hybridization testing
Classification

Lymph node with mantle cell lymphoma (low-power view, H&E)
Lymphomas in the strict sense are any neoplasms of the lymphatic tissues (lympho- + -oma) .[23] The main classes are malignant neoplasms (that is, cancers) of the lymphocytes, a type of white blood cell that belongs to both the lymph and the blood and pervades both. Thus, lymphomas and leukemias are both tumors of the hematopoietic and lymphoid tissues, and as lymphoproliferative disorders, lymphomas and lymphoid leukemias are closely related, to the point that some of them are unitary disease entities that can be called by either name (for example adult T-cell leukemia/lymphoma).
Several classification systems have existed for lymphoma, which use histological and other findings to divide lymphoma into different categories. The classification of a lymphoma can affect treatment and prognosis. Classification systems generally classify lymphoma according to:
- Whether or not it is a Hodgkin lymphoma
- Whether the cell that is replicating is a T cell or B cell
- The site from which the cell arises
Lymphoma can also spread to the central nervous system, often around the brain in the meninges, known as lymphomatous meningitis (LM).[24]
Hodgkin lymphoma
Hodgkin lymphoma accounts for about 15% of lymphomas.[25] It differs from other forms of lymphoma in its prognosis and several pathological characteristics. A division into Hodgkin and non-Hodgkin lymphomas is used in several of the older classification systems. A Hodgkin lymphoma is marked by the presence of a type of cell called the Reed–Sternberg cell.[26][27]
Non-Hodgkin lymphomas
Non-Hodgkin lymphomas, which are defined as being all lymphomas except Hodgkin lymphoma, are more common than Hodgkin lymphoma. A wide variety of lymphomas are in this class, and the causes, the types of cells involved, and the prognosis vary by type. The incidence of non-Hodgkin lymphoma increases with age.
It is further divided into several subtypes.
Epstein-Barr virus-associated lymphoproliferative diseases
Epstein-Barr virus-associated lymphoproliferative diseases are a group of benign, pre-malignant, and malignant diseases of lymphoid cells, i.e. B cells, T cells, NK cells, and histiocytic-dendritic cells in which one or more of these cell types is infected with the Epstein-Barr virus (EBV). The virus may be responsible for the development and/or progression of these diseases. In addition to EBV-positive Hodgkin lymphomas, the World Health Organization (2016) includes the following lymphomas, when associated with EBV infection, in this group of diseases: Burkitt lymphoma; large B cell lymphoma, not otherwise specified; diffuse large B cell lymphoma associated with chronic inflammation; fibrin-associated diffuse large cell lymphoma; primary effusion lymphoma; plasmablastic lymphoma; extranodal NK/T cell lymphoma, nasal type; peripheral T cell lymphoma, not otherwise specified; angioimmunoblastic T cell lymphoma; follicular T cell lymphoma; and systemic T cell lymphoma of childhood.[28]
WHO classification
The WHO classification, published in 2001 and updated in 2008,[29][30] is based upon the foundations laid within the "revised European-American lymphoma classification" (REAL). This system groups lymphomas by cell type (i.e. the normal cell type that most resembles the tumor) and defining phenotypic, molecular, or cytogenetic characteristics. The five groups are shown in the table. Hodgkin lymphoma is considered separately within the WHO and preceding classifications, although it is recognized as being a tumor of, albeit markedly abnormal, lymphocytes of mature B cell lineage.
Of the many forms of lymphoma, some are categorized as indolent (e.g. small lymphocytic lymphoma), compatible with a long life even without treatment, whereas other forms are aggressive (e.g. Burkitt's lymphoma), causing rapid deterioration and death. However, most of the aggressive lymphomas respond well to treatment and are curable. The prognosis, therefore, depends on the correct diagnosis and classification of the disease, which is established after examination of a biopsy by a pathologist (usually a hematopathologist).[31]

DNA-microarray analysis of Burkitt's lymphoma and diffuse large B-cell lymphoma (DLBCL) showing differences in gene expression patterns. Colors indicate levels of expression; green indicates genes that are underexpressed in lymphoma cells (as compared to normal cells), whereas red indicates genes that are overexpressed in lymphoma cells.
- B-cell chronic lymphocytic leukemia/small cell lymphoma
- 3 to 4% of lymphomas in adults
- Small resting lymphocytes mixed with variable numbers of large activated cells, lymph nodes diffusely effaced
- CD5, surface immunoglobulin
- 50%.[32]
- Occurs in older adults, usually involves lymph nodes, bone marrow and spleen, most patients have peripheral blood involvement, indolent
- B-cell prolymphocytic leukemia
Lymphoplasmacytic lymphoma (such as Waldenström macroglobulinemia)- Splenic marginal zone lymphoma
- Hairy cell leukemia
Plasma cell neoplasms:
Plasma cell myeloma (also known as multiple myeloma)- Plasmacytoma
- Monoclonal immunoglobulin deposition diseases
- Heavy chain diseases
Extranodal marginal zone B cell lymphoma, also called MALT lymphoma
- About 5% of lymphomas in adults
- Variable cell size and differentiation, 40% show plasma cell differentiation, homing of B cells to epithelium creates lymphoepithelial lesions.
- CD5, CD10, surface Ig
- Frequently occurs outside lymph nodes, very indolent, may be cured by local excision
- Nodal marginal zone B cell lymphoma
- Follicular lymphoma
- About 40% of lymphomas in adults
- Small "cleaved" cells (centrocytes) mixed with large activated cells (centroblasts), usually nodular ("follicular") growth pattern
CD10, surface Ig
- 72–77%[33]
- Occurs in older adults, usually involves lymph nodes, bone marrow and spleen, associated with t(14;18) translocation overexpressing Bcl-2, indolent
- Primary cutaneous follicle center lymphoma
- Mantle cell lymphoma
- 3 to 4% of lymphomas in adults
- Lymphocytes of small to intermediate size growing in diffuse pattern
- CD5
- 50%[34] to 70%[34]
- Occurs mainly in adult males, usually involves lymph nodes, bone marrow, spleen and GI tract, associated with t(11;14) translocation overexpressing cyclin D1, moderately aggressive
Diffuse large B cell lymphoma, not otherwise specified
- About 40 to 50% of lymphomas in adults
- Variable, most resemble B cells of large germinal centers, diffuse growth pattern
- Variable expression of CD10 and surface Ig
5-year survival 60%[35]
- Occurs in all ages, but most commonly in older adults, may occur outside lymph nodes, aggressive
- Diffuse large B-cell lymphoma associated with chronic inflammation
- Epstein–Barr virus-positive DLBCL of the elderly
- Lymphomatoid granulomatosis
- Primary mediastinal (thymic) large B-cell lymphoma
- Intravascular large B-cell lymphoma
- ALK+ large B-cell lymphoma
- Plasmablastic lymphoma
- Primary effusion lymphoma
- Large B-cell lymphoma arising in HHV8-associated multicentric Castleman's disease
- Burkitt lymphoma/leukemia
- < 1% of lymphomas in the United States
- Round lymphoid cells of intermediate size with several nucleoli, starry-sky appearance by diffuse spread with interspersed apoptosis
- CD10, surface Ig
5-year
survival 50%[36]
- Endemic in Africa, sporadic elsewhere, more common in immunocompromised and children, often visceral involvement, highly aggressive
- T-cell prolymphocytic leukemia
- T-cell large granular lymphocyte leukemia
- Aggressive NK cell leukemia
- Adult T-cell leukemia/lymphoma
- Extranodal NK/T-cell lymphoma, nasal type
- Enteropathy-associated T-cell lymphoma
- Hepatosplenic T-cell lymphoma
- Blastic NK cell lymphoma
Mycosis fungoides / Sezary syndrome
- Most common cutaneous lymphoid malignancy
- Usually small lymphoid cells with convoluted nuclei that often infiltrate the epidermis, creating Pautrier microabscesseses
- CD4
5-year
survival 75%[37]
- Localized or more generalized skin symptoms, generally indolent, in a more aggressive variant, Sézary's disease, skin erythema and peripheral blood involvement
- Primary cutaneous CD30-positive T cell lymphoproliferative disorders
- Primary cutaneous anaplastic large cell lymphoma
- Lymphomatoid papulosis
- Peripheral T-cell lymphoma not otherwise specified
- Most common T cell lymphoma
- Variable, usually a mix small to large lymphoid cells with irregular nuclear contours
- CD3
- Probably consists of several rare tumor types, often disseminated and generally aggressive
- Angioimmunoblastic T cell lymphoma
- Anaplastic large cell lymphoma
- B-lymphoblastic leukemia/lymphoma not otherwise specified
- B-lymphoblastic leukemia/lymphoma with recurrent genetic abnormalities
- T-lymphoblastic leukemia/lymphoma
- 15% of childhood acute lymphoblastic leukemia and 90% of lymphoblastic lymphoma.[29]:635
Lymphoblasts with irregular nuclear contours, condensed chromatin, small nucleoli and scant cytoplasm without granules
TdT, CD2, CD7
- It often presents as a mediastinal mass because of involvement of the thymus. It is highly associated with NOTCH1 mutations, and is most common in adolescent males.
- 15% of childhood acute lymphoblastic leukemia and 90% of lymphoblastic lymphoma.[29]:635
- Classical Hodgkin lymphomas:
Nodular sclerosis form of Hodgkin lymphoma
- Most common type of Hodgkin lymphoma
- Reed-Sternberg cell variants and inflammation, usually broad sclerotic bands that consist of collagen
CD15, CD30
- Most common in young adults, often arises in the mediastinum or cervical lymph nodes
- Mixed cellularity Hodgkin lymphoma
- Second-most common form of Hodgkin lymphoma
- Many classic Reed-Sternberg cells and inflammation
- CD15, CD30
- Most common in men, more likely to be diagnosed at advanced stages than the nodular sclerosis form Epstein-Barr virus involved in 70% of cases
- Lymphocyte-rich
- Lymphocyte depleted or not depleted
- Nodular lymphocyte-predominant Hodgkin lymphoma
- Associated with a primary immune disorder
- Associated with the human immunodeficiency virus (HIV)
- Post-transplant
- Associated with methotrexate therapy
Primary central nervous system lymphoma occurs most often in immunocompromised patients, in particular those with AIDS, but it can occur in the immunocompetent, as well. It has a poor prognosis, particularly in those with AIDS. Treatment can consist of corticosteroids, radiotherapy, and chemotherapy, often with methotrexate.
Previous classifications
Several previous classifications have been used, including Rappaport 1956, Lennert / Kiel 1974, BNLI, Working formulation (1982), and REAL (1994).
The Working formulation of 1982 was a classification of non-Hodgkin lymphoma. It excluded the Hodgkin lymphomas and divided the remaining lymphomas into four grades (low, intermediate, high, and miscellaneous) related to prognosis, with some further subdivisions based on the size and shape of affected cells. This purely histological classification included no information about cell surface markers, or genetics, and it made no distinction between T-cell lymphomas and B-cell lymphomas. It was widely accepted at the time of its publication, but is now obsolete.[38] It is still used by some cancer agencies for compilation of lymphoma statistics and historical rate comparisons.[citation needed]
In 1994, the Revised European-American Lymphoma (REAL) classification applied immunophenotypic and genetic features in identifying distinct clinicopathologic entities among all the lymphomas except Hodgkin lymphoma.[39] For coding purposes, the ICD-O (codes 9590–9999)[40] and ICD-10 (codes C81-C96)[41] are available.
Staging

Diagram showing common sites where lymphoma spreads
After a diagnosis and before treatment, a cancer is staged. This refers to determining if the cancer has spread, and if so, whether locally or to distant sites. Staging is reported as a grade between I (confined) and IV (spread). Staging is carried out because the stage of a cancer impacts its prognosis and treatment.[citation needed]
The Ann Arbor staging system is routinely used for staging of both HL and NHL. In this staging system, I represents a localised disease contained within a lymph node group, II represents the presence of lymphoma in two or more lymph nodes groups, III represents spread of the lymphoma to lymph nodes groups on both sides of the diaphragm, and IV indicates spread to tissue outside the lymphatic system. Different suffixes imply involvement of different organs, for example S for the spleen and H for the liver. Extra-lymphatic involvement is expressed with the letter E.
In addition, the presence of B symptoms or their absence is expressed with B and A, respectively. B symptoms are defined as the presence of one of three symptoms: Unintentional weightloss of 10% body weight in the last 6 months, night sweats, and persistent fever of 38 °C or more.[42]
CT scan or PET scan imaging modalities are used to stage a cancer. PET scan is advised for FDG avid lymphomas, for example Hodgkins Lymphoma as a staging tool that can even replace bone marrow biopsy. For other lymphomas CT scan is recommended for staging.[43]
Age and poor performance status are established poor prognostic factors, as well.[44]
Mantle cell lymphoma: Notice the irregular nuclear contours of the medium-sized lymphoma cells and the presence of a pink histiocyte. By immunohistochemistry, the lymphoma cells expressed CD20, CD5, and Cyclin D1 (high-power view, H&E)

Hodgkin lymphoma, nodular lymphocyte predominant (low-power view): Notice the nodular architecture and the areas of "mottling".(H&E)

Hodgkin lymphoma, nodular lymphocyte predominant (high-power view): Notice the presence of L&H cells, also known as "popcorn cells". (H&E)



Differential diagnosis
Certain lymphomas (extranodal NK/T-cell lymphoma, nasal type and type II enteropathy-associated T-cell lymphoma) can be mimicked by two benign diseases which involve the excessive proliferation of non-malignant NK cells in the GI tract, natural killer cell enteropathy, a disease wherein NK cell infiltrative lesions occur in the intestine, colon, stomach, or esophagus, and lymphomatoid gastropathy, a disease wherein these cells' infiltrative lesions are limited to the stomach. These diseases do not progress to cancer, may regress spontaneously and do not respond to, and do not require, chemotherapy or other lymphoma treatments.[45]
Treatment
Prognoses and treatments are different for HL and between all the different forms of NHL,[46] and also depend on the grade of tumour, referring to how quickly a cancer replicates. Paradoxically, high-grade lymphomas are more readily treated and have better prognoses:[citation needed]Burkitt lymphoma, for example, is a high-grade tumour known to double within days, and is highly responsive to treatment. Lymphomas may be curable if detected in early stages with modern treatment.
Low-grade
Many low-grade lymphomas remain indolent for many years. Treatment of the nonsymptomatic patient is often avoided. In these forms of lymphoma, such as follicular lymphoma, watchful waiting is often the initial course of action. This is carried out because the harms and risks of treatment outweigh the benefits.[47] If a low-grade lymphoma is becoming symptomatic, radiotherapy or chemotherapy are the treatments of choice; although they do not cure the lymphoma, they can alleviate the symptoms, particularly painful lymphadenopathy. Patients with these types of lymphoma can live near-normal lifespans, but the disease is incurable. Some centers advocate the use of single agent rituximab in the treatment of follicular lymphoma rather than the wait and watch approach. Watchful waiting is not a good strategy for all patients, as it leads to significant distress and anxiety in some patients. It has been equated with watch and worry.[48]
High-grade
Treatment of some other, more aggressive, forms of lymphoma[which?] can result in a cure in the majority of cases, but the prognosis for patients with a poor response to therapy is worse.[49] Treatment for these types of lymphoma typically consists of aggressive chemotherapy, including the CHOP or R-CHOP regimen. A number of people are cured with first-line chemotherapy. Most relapses occur within the first two years, and the relapse risk drops significantly thereafter.[50] For people who relapse, high-dose chemotherapy followed by autologous stem cell transplantation is a proven approach.[51]
Hodgkin lymphoma
Hodgkin lymphoma typically is treated with radiotherapy alone, as long as it is localized.[52]
Advanced Hodgkin disease requires systemic chemotherapy, sometimes combined with radiotherapy.[53] Chemotherapy used includes the ABVD regimen, which is commonly used in the United States. Other regimens used in the management of Hodgkin lymphoma include BEACOPP and Stanford V. Considerable controversy exists regarding the use of ABVD or BEACOPP. Briefly, both regimens are effective, but BEACOPP is associated with more toxicity. Encouragingly, a significant number of people who relapse after ABVD can still be salvaged by stem cell transplant.[54]
Palliative care
Palliative care, a specialized medical care focused on the symptoms, pain, and stress of a serious illness, is recommended by multiple national cancer treatment guidelines as an accompaniment to curative treatments for people suffering from lymphoma.[55][56] It is used to address both the direct symptoms of lymphoma and many unwanted side effects that arise from treatments.[57][58] Palliative care can be especially helpful for children who develop lymphoma, helping both children and their families deal with the physical and emotional symptoms of the disease.[57][59][60][61] For these reasons, palliative care is especially important for patients requiring bone marrow transplants.[62][63]
Prognosis
| Five-year relative survival by stage at diagnosis[64] | ||
| Stage at diagnosis | Five-year relative survival (%) | Percentage of cases (%) |
| Localized (confined to primary site) | 82.3 | 26 |
| Regional (spread to regional lymph nodes) | 78.3 | 19 |
| Distant (cancer has metastasized) | 62.7 | 47 |
| Unknown (unstaged) | 68.6 | 8 |
Epidemiology

Deaths from lymphomas and multiple myeloma per million persons in 2012 .mw-parser-output .refbegin{font-size:90%;margin-bottom:0.5em}.mw-parser-output .refbegin-hanging-indents>ul{list-style-type:none;margin-left:0}.mw-parser-output .refbegin-hanging-indents>ul>li,.mw-parser-output .refbegin-hanging-indents>dl>dd{margin-left:0;padding-left:3.2em;text-indent:-3.2em;list-style:none}.mw-parser-output .refbegin-100{font-size:100%}
0-13
14-18
19-22
23-28
29-34
35-42
43-57
58-88
89-121
122-184
Lymphoma is the most common form of hematological malignancy, or "blood cancer", in the developed world.
Taken together, lymphomas represent 5.3% of all cancers (excluding simple basal cell and squamous cell skin cancers) in the United States and 55.6% of all blood cancers.[65]
According to the U.S. National Institutes of Health, lymphomas account for about 5%, and Hodgkin lymphoma in particular accounts for less than 1% of all cases of cancer in the United States.
Because the whole system is part of the body's immune system, patients with a weakened immune system such as from HIV infection or from certain drugs or medication also have a higher incidence of lymphoma.[66]
History

Thomas Hodgkin
Thomas Hodgkin published the first description of lymphoma in 1832, specifically of the form named after him.[67] Since then, many other forms of lymphoma have been described.
Research
The two types of lymphoma research are clinical or translational research and basic research. Clinical/translational research focuses on studying the disease in a defined and generally immediately patient-applicable way, such as testing a new drug in patients. Studies may focus on effective means of treatment, better ways of treating the disease, improving the quality of life for patients, or appropriate care in remission or after cures. Hundreds of clinical trials are being planned or conducted at any given time.[68]
Basic science research studies the disease process at a distance, such as seeing whether a suspected carcinogen can cause healthy cells to turn into lymphoma cells in the laboratory or how the DNA changes inside lymphoma cells as the disease progresses. The results from basic research studies are generally less immediately useful to patients with the disease,[69] but can improve scientists' understanding of lymphoma and form the foundation for future, more effective treatments.
Other animals
References
^ abcdefghijk "General Information About Adult Hodgkin Lymphoma". National Cancer Institute. 2014-04-23. Archived from the original on 5 July 2014. Retrieved 20 June 2014..mw-parser-output cite.citation{font-style:inherit}.mw-parser-output .citation q{quotes:"""""""'""'"}.mw-parser-output .citation .cs1-lock-free a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/6/65/Lock-green.svg/9px-Lock-green.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .citation .cs1-lock-limited a,.mw-parser-output .citation .cs1-lock-registration a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/d/d6/Lock-gray-alt-2.svg/9px-Lock-gray-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .citation .cs1-lock-subscription a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/a/aa/Lock-red-alt-2.svg/9px-Lock-red-alt-2.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration{color:#555}.mw-parser-output .cs1-subscription span,.mw-parser-output .cs1-registration span{border-bottom:1px dotted;cursor:help}.mw-parser-output .cs1-ws-icon a{background:url("//upload.wikimedia.org/wikipedia/commons/thumb/4/4c/Wikisource-logo.svg/12px-Wikisource-logo.svg.png")no-repeat;background-position:right .1em center}.mw-parser-output code.cs1-code{color:inherit;background:inherit;border:inherit;padding:inherit}.mw-parser-output .cs1-hidden-error{display:none;font-size:100%}.mw-parser-output .cs1-visible-error{font-size:100%}.mw-parser-output .cs1-maint{display:none;color:#33aa33;margin-left:0.3em}.mw-parser-output .cs1-subscription,.mw-parser-output .cs1-registration,.mw-parser-output .cs1-format{font-size:95%}.mw-parser-output .cs1-kern-left,.mw-parser-output .cs1-kern-wl-left{padding-left:0.2em}.mw-parser-output .cs1-kern-right,.mw-parser-output .cs1-kern-wl-right{padding-right:0.2em}
^ abcdefghijklmn "General Information About Adult Non-Hodgkin Lymphoma". National Cancer Institute. 2014-04-25. Archived from the original on 5 July 2014. Retrieved 20 June 2014.
^ ab Kamper-Jørgensen, M; Rostgaard, K; Glaser, SL; Zahm, SH; Cozen, W; Smedby, KE; Sanjosé, S; Chang, ET; Zheng, T; La Vecchia, C; Serraino, D; Monnereau, A; Kane, EV; Miligi, L; Vineis, P; Spinelli, JJ; McLaughlin, JR; Pahwa, P; Dosman, JA; Vornanen, M; Foretova, L; Maynadie, M; Staines, A; Becker, N; Nieters, A; Brennan, P; Boffetta, P; Cocco, P; Hjalgrim, H (September 2013). "Cigarette smoking and risk of Hodgkin lymphoma and its subtypes: a pooled analysis from the International Lymphoma Epidemiology Consortium (InterLymph)". Annals of Oncology. 24 (9): 2245–55. doi:10.1093/annonc/mdt218. PMC 3755332. PMID 23788758.
^ ab "Hodgkin Lymphoma—SEER Stat Fact Sheets". Seer.cancer.gov. Archived from the original on 2012-10-17. Retrieved 2012-08-26.
^ GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
^ GBD 2015 Mortality and Causes of Death, Collaborators. (8 October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
^ ab Taylor, Elizabeth J. (2000). Dorland's Illustrated medical dictionary (29th ed.). Philadelphia: Saunders. p. 1038. ISBN 0721662544.
^ Aditya Bardia (2010). Johns Hopkins Patients' Guide to Lymphoma. Jones & Bartlett Learning. p. 6. ISBN 9781449631413. Archived from the original on 2017-09-10.
^ abc The Lymphoma Guide Information for Patients and Caregivers (pdf). Leukemia and Lymphoma Society. 2013. Archived (PDF) from the original on 14 July 2014. Retrieved 20 June 2014.
^ abcd World Cancer Report 2014. World Health Organization. 2014. pp. Chapter 5.13. ISBN 9283204298.
^ "Lymphoma". NCI. Archived from the original on 5 July 2014. Retrieved 13 June 2014.
^ Vardiman JW, Thiele J, Arber DA, Brunning RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM, Hellström-Lindberg E, Tefferi A, Bloomfield CD (Jul 30, 2009). "The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes". Blood. 114 (5): 937–51. doi:10.1182/blood-2009-03-209262. PMID 19357394.
^ Hu, L; Luo, D; Zhou, T; Tao, Y; Feng, J; Mei, S (12 August 2017). "The association between non-Hodgkin lymphoma and organophosphate pesticides exposure: A meta-analysis". Environmental pollution (Barking, Essex : 1987). 231 (Pt 1): 319–328. doi:10.1016/j.envpol.2017.08.028. PMID 28810201.
^ Yang, L; Dong, J; Jiang, S; Shi, W; Xu, X; Huang, H; You, X; Liu, H (November 2015). "Red and Processed Meat Consumption Increases Risk for Non-Hodgkin Lymphoma: A PRISMA-Compliant Meta-Analysis of Observational Studies". Medicine. 94 (45): e1729. doi:10.1097/MD.0000000000001729. PMC 4912242. PMID 26559248.
^ Solimini, AG; Lombardi, AM; Palazzo, C; De Giusti, M (May 2016). "Meat intake and non-Hodgkin lymphoma: a meta-analysis of observational studies". Cancer Causes & Control. 27 (5): 595–606. doi:10.1007/s10552-016-0745-2. PMID 27076059.
^ "SEER Stat Fact Sheets: Non-Hodgkin Lymphoma". NCI. Archived from the original on 6 July 2014. Retrieved 18 June 2014.
^ Marcus, Robert (2013). Lymphoma : pathology, diagnosis and treatment (Second ed.). p. 1. ISBN 9781107010598. Archived from the original on 2015-09-06.
^ Tepper, John E. Niederhuber, James O. Armitage, James H. Doroshow, Michael B. Kastan, Joel E. (2014). "Childhood lymphoma". Abeloff's clinical oncology (Fifth ed.). p. Chapter 97. ISBN 1455728659.
^ abcdef "About Lymphoma". Lymphoma Research Foundation. Archived from the original on 2 December 2012. Retrieved 22 December 2012.
^ abcdefgh "Warning Signs of Lymphoma — First Signs of Lymphoma". Lymphoma.about.com. Archived from the original on 2012-11-18. Retrieved 2012-12-01.
^ Subhaschandra Singh, Y. Sobita Devi, Shweta Bhalothia and Veeraraghavan Gunasekaran (2016). "Peritoneal Carcinomatosis: Pictorial Review of Computed Tomography Findings". International Journal of Advanced Research. 4 (7): 735–748. doi:10.21474/IJAR01/936. ISSN 2320-5407.CS1 maint: Multiple names: authors list (link)
CC-BY 4.0
^ Mallick, Indranil. "How Is Lymphoma Diagnosed?". lymphoma.about.com. Archived from the original on 16 January 2013. Retrieved 22 December 2012.
^ Elsevier, Dorland's Illustrated Medical Dictionary, Elsevier.
^ Canova, F; Marino, D; Trentin, C; Soldà, C; Ghiotto, C; Aversa, SM (August 2011). "Intrathecal chemotherapy in lymphomatous meningitis". Critical reviews in oncology/hematology. 79 (2): 127–34. doi:10.1016/j.critrevonc.2010.07.005. PMID 20696592.
^ "Hodgkins Lymphoma Incidence". Retrieved 2 October 2017.
^ National Cancer Institute, "Hodgkin Lymphoma", "Archived copy". Archived from the original on 2013-08-02. Retrieved 2013-08-05.CS1 maint: Archived copy as title (link), accessed on 2013-08-05
^ National Cancer Institute. "What You Need To Know About Hodgkin Lymphoma". U.S. Dept of Health and Human Services, (online at "Archived copy" (PDF). Archived from the original (PDF) on 2014-01-24. Retrieved 2013-08-05.CS1 maint: Archived copy as title (link)), pg 4.
^ Rezk SA, Zhao X, Weiss LM (June 2018). "Epstein - Barr virus - associated lymphoid proliferations, a 2018 update". Human Pathology. doi:10.1016/j.humpath.2018.05.020. PMID 29885408.
^ ab Jaffe, ES; Harris, NL; Vardiman, JW; Campo, E; Arber, DA. (2011). Hematopathology (1st ed.). Elsevier Saunders. ISBN 9780721600406.
^ Swerdlow, Steven H.; International Agency for Research on Cancer; World Health Organization (2008). WHO classification of tumours of haematopoietic and lymphoid tissues. World Health Organization classification of tumours. 2 (4th ed.). International Agency for Research on Cancer. ISBN 9789283224310. Archived from the original on 2015-02-11.
^ Wagman LD. (2008). "Principles of Surgical Oncology". In Pazdur R, Wagman LD, Camphausen KA, Hoskins WJ. Cancer Management: A Multidisciplinary Approach (11th ed.). CMPMedica. ISBN 9781891483622. Archived from the original on 2013-10-04.
^ "Chronic Leukemias". The Merck Manual of Geriatrics. Archived from the original on 2010-07-04.
^ Lymphoma, Follicular at eMedicine
^ ab
- 50% for limited stage: Leitch HA, Gascoyne RD, Chhanabhai M, Voss NJ, Klasa R, Connors JM (October 2003). "Limited-stage mantle-cell lymphoma". Ann. Oncol. 14 (10): 1555–61. doi:10.1093/annonc/mdg414. PMID 14504058.
- 70% for advanced stage: Herrmann A, Hoster E, Zwingers T, Brittinger G, Engelhard M, Meusers P, Reiser M, Forstpointner R, Metzner B, Peter N, Wörmann B, Trümper L, Pfreundschuh M, Einsele H, Hiddemann W, Unterhalt M, Dreyling M (February 2009). "Improvement of overall survival in advanced stage mantle cell lymphoma". J. Clin. Oncol. 27 (4): 511–8. doi:10.1200/JCO.2008.16.8435. PMID 19075279.
- 50% for limited stage: Leitch HA, Gascoyne RD, Chhanabhai M, Voss NJ, Klasa R, Connors JM (October 2003). "Limited-stage mantle-cell lymphoma". Ann. Oncol. 14 (10): 1555–61. doi:10.1093/annonc/mdg414. PMID 14504058.
^ Turgeon, Mary Louise (2005). Clinical Hematology: Theory and Procedures. 936 (4 ed.). Lippincott Williams & Wilkins. pp. 285–6. ISBN 978-0-7817-5007-3. Archived from the original on 2015-09-06.
^ Diviné M, Casassus P, Koscielny S, Bosq J, Sebban C, Le Maignan C, Stamattoulas A, Dupriez B, Raphaël M, Pico JL, Ribrag V (December 2005). "Burkitt lymphoma in adults: a prospective study of 72 patients treated with an adapted pediatric LMB protocol". Ann. Oncol. 16 (12): 1928–35. doi:10.1093/annonc/mdi403. PMID 16284057.
^ Kirova YM, Piedbois Y, Haddad E, Levy E, Calitchi E, Marinello G, Le Bourgeois JP (May 1999). "Radiotherapy in the management of mycosis fungoides: indications, results, prognosis. Twenty years experience". Radiother Oncol. 51 (2): 147–51. doi:10.1016/S0167-8140(99)00050-X. PMID 10435806.
^ Clarke CA, Glaser SL, Dorfman RF, Bracci PM, Eberle E, Holly EA (January 2004). "Expert review of non-Hodgkin lymphomas in a population-based cancer registry: reliability of diagnosis and subtype classifications". Cancer Epidemiol. Biomarkers Prev. 13 (1): 138–43. doi:10.1158/1055-9965.EPI-03-0250. PMID 14744745.
^ Non-Hodgkin Lymphoma at eMedicine
^ "Archived copy". Archived from the original on June 27, 2004. Retrieved 2005-11-07.CS1 maint: Archived copy as title (link) CS1 maint: BOT: original-url status unknown (link)
^ who.int
^ Report of the Committee on Hodgkin's Disease Staging Classification
Paul P. Carbone (Chairman), Henry S. Kaplan, Karl Musshoff, David W. Smithers, and Maurice Tubing,[CANCER RESEARCH 31, 1860- 1861, November 1971]
^ Staging and response assessment in lymphomas: the new Lugano classification,Bruce D. Cheson.Chin Clin Oncol 2015:4(1):5
^ International Prognostic Index N Engl J Med. 1993;329(14):987–94
^ Xia D, Morgan EA, Berger D, Pinkus GS, Ferry JA, Zukerberg LR (January 2019). "NK-Cell Enteropathy and Similar Indolent Lymphoproliferative Disorders: A Case Series With Literature Review". American Journal of Clinical Pathology. 151 (1): 75–85. doi:10.1093/ajcp/aqy108. PMID 30212873.
^ Sweetenham JW (November 2009). "Treatment of lymphoblastic lymphoma in adults". Oncology (Williston Park, N.Y.). 23 (12): 1015–20. PMID 20017283.
^ Elphee EE (May 2008). "Understanding the concept of uncertainty in patients with indolent lymphoma". Oncol Nurs Forum. 35 (3): 449–54. doi:10.1188/08.ONF.449-454. PMID 18467294.
^ Ansell SM (2014). "Follicular lymphoma: Watch and wait is watch and worry". The Lancet Oncology. 15 (4): 368–9. doi:10.1016/S1470-2045(14)70066-X. PMID 24602759.
^ Bernstein SH, Burack WR; Burack (2009). "The incidence, natural history, biology, and treatment of transformed lymphomas". Hematology Am Soc Hematol Educ Program. 2009: 532–41. doi:10.1182/asheducation-2009.1.532. PMID 20008238.
^ Jenkins EC (Jan 1972). "Wire-loop application of liquid emulsion to slides for autoradiography in light microscopy". Stain technology. 47 (1): 23–6. doi:10.3109/10520297209116530. PMID 4550425.
^ Philip T, Guglielmi C, Hagenbeek A, Somers R, Van der Lelie H, Bron D, Sonneveld P, Gisselbrecht C, Cahn JY, Harousseau JL (Dec 7, 1995). "Autologous bone marrow transplantation as compared with salvage chemotherapy in relapses of chemotherapy-sensitive non-Hodgkin's lymphoma". The New England Journal of Medicine. 333 (23): 1540–5. doi:10.1056/nejm199512073332305. PMID 7477169.
^ Martin NE, Ng AK; Ng (November 2009). "Good things come in small packages: low-dose radiation as palliation for indolent non-Hodgkin lymphomas". Leuk. Lymphoma. 50 (11): 1765–72. doi:10.3109/10428190903186510. PMID 19883306.
^ Kuruvilla J (2009). "Standard therapy of advanced Hodgkin lymphoma". Hematology Am Soc Hematol Educ Program. 2009: 497–506. doi:10.1182/asheducation-2009.1.497. PMID 20008235.
^ Viviani S, Zinzani PL, Rambaldi A, Brusamolino E, Levis A, Bonfante V, Vitolo U, Pulsoni A, Liberati AM, Specchia G, Valagussa P, Rossi A, Zaja F, Pogliani EM, Pregno P, Gotti M, Gallamini A, Rota Scalabrini D, Bonadonna G, Gianni AM (2011). "ABVD versus BEACOPP for Hodgkin's lymphoma when high-dose salvage is planned". New England Journal of Medicine. 365 (3): 203–12. doi:10.1056/NEJMoa1100340. PMID 21774708.
^ Ferrell B, Connor SR, Cordes A, Dahlin CM, Fine PG, Hutton N, Leenay M, Lentz J, Person JL, Meier DE, Zuroski K (2007). "The national agenda for quality palliative care: the National Consensus Project and the National Quality Forum". J Pain Symptom Manage. 33 (6): 737–44. doi:10.1016/j.jpainsymman.2007.02.024. PMID 17531914.
^ *The American Society of Clinical Oncology made this recommendation based on various cancers. See American Society of Clinical Oncology, "Five Things Physicians and Patients Should Question" (PDF), Choosing Wisely: an initiative of the ABIM Foundation, American Society of Clinical Oncology, archived from the original (PDF) on July 31, 2012, retrieved August 14, 2012
^ ab Higginson IJ, Evans CJ; Evans (2010). "What is the evidence that palliative care teams improve outcomes for cancer patients and their families?". Cancer J. 16 (5): 423–35. doi:10.1097/PPO.0b013e3181f684e5. PMID 20890138.
^ "Palliative Care: It's for Caregivers Too, Says Study". Archived from the original on 2014-06-01. Retrieved 2014-08-21.
^ Heath JA, Clarke NE, Donath SM, McCarthy M, Anderson VA, Wolfe J (2010). "Symptoms and suffering at the end of life in children with cancer: an Australian perspective". Med J Aust. 192 (2): 71–5. PMID 20078405.
^ Schmidt P, Otto M, Hechler T, Metzing S, Wolfe J, Zernikow B (2013). "Did increased availability of pediatric palliative care lead to improved palliative care outcomes in children with cancer?". J Palliat Med. 16 (9): 1034–9. doi:10.1089/jpm.2013.0014. PMID 23901834.
^ Tang ST, Chang WC, Chen JS, Wang HM, Shen WC, Li CY, Liao YC (2013). "Course and predictors of depressive symptoms among family caregivers of terminally ill cancer patients until their death". Psychooncology. 22 (6): 1312–8. doi:10.1002/pon.3141. PMID 22836818.
^ Chung HM, Lyckholm LJ, Smith TJ (2009). "Palliative care in BMT". Bone Marrow Transplant. 43 (4): 265–73. doi:10.1038/bmt.2008.436. PMID 19151797.
^ "Providing Palliative Care to Family Caregivers Throughout the Bone Marrow Transplantation Trajectory". Archived from the original on 2013-08-12. Retrieved 2014-08-21.
^ "SEER Stat Fact Sheets: Lymphoma". Archived from the original on 2013-10-10.
^ Horner MJ, Ries LG, Krapcho M, Neyman N. "SEER Cancer Statistics Review, 1975–2006". Surveillance Epidemiology and End Results (SEER). Bethesda, MD: National Cancer Institute. Archived from the original on 26 September 2009. Retrieved 3 November 2009.Table 1.4: Age-Adjusted SEER Incidence and U.S. Death Rates and 5-Year Relative Survival Rates By Primary Cancer Site, Sex and Time Period
^ Tran H, Nourse J, Hall S, Green M, Griffiths L, Gandhi MK (Sep 2008). "Immunodeficiency-associated lymphomas". Blood Reviews. 22 (5): 261–281. doi:10.1016/j.blre.2008.03.009. PMID 18456377.
^ Hellman, Samuel; Mauch, P.M. Ed. (1999). Hodgkin's Disease. Chapter 1: Lippincott Williams & Wilkins. p. 5. ISBN 0-7817-1502-4.
^ "Archived copy". Archived from the original on 2013-01-06. Retrieved 2012-10-30.CS1 maint: Archived copy as title (link)
^ "Understanding Clinical Trials for Blood Cancers" (PDF). The Leukemia & Lymphoma Society. Leukemia and Lymphoma Society. Archived from the original (pdf) on 5 January 2011. Retrieved 19 May 2010.
External links
| Classification | D
|
|---|---|
| External resources |
|
Lymphoma at Curlie


