Alzheimer's disease
| Alzheimer's disease | |
|---|---|
| Synonyms | Alzheimer disease, Alzheimer's |
 | |
| Comparison of a normal aged brain (left) and the brain of a person with Alzheimer's (right). Characteristics that separate the two are pointed out. | |
| Specialty | Neurology |
| Symptoms | Difficulty in remembering recent events, problems with language, disorientation, mood swings[1][2] |
| Usual onset | Over 65 years old[3] |
| Duration | Long term[2] |
| Causes | Poorly understood[1] |
| Risk factors | Genetics, head injuries, depression, hypertension[1][4] |
| Diagnostic method | Based on symptoms and cognitive testing after ruling out other possible causes[5] |
| Differential diagnosis | Normal aging[1] |
| Medication | Acetylcholinesterase inhibitors, NMDA receptor antagonists (small benefit)[6] |
| Prognosis | Life expectancy 3–9 years[7] |
| Frequency | 29.8 million (2015)[2][8] |
| Deaths | 1.9 million (2015)[9] |
Alzheimer's disease (AD), also referred to simply as Alzheimer's, is a chronic neurodegenerative disease that usually starts slowly and worsens over time.[1][2] It is the cause of 60–70% of cases of dementia.[1][2] The most common early symptom is difficulty in remembering recent events (short-term memory loss).[1] As the disease advances, symptoms can include problems with language, disorientation (including easily getting lost), mood swings, loss of motivation, not managing self care, and behavioural issues.[1][2] As a person's condition declines, they often withdraw from family and society.[1] Gradually, bodily functions are lost, ultimately leading to death.[10] Although the speed of progression can vary, the typical life expectancy following diagnosis is three to nine years.[7][11]
The cause of Alzheimer's disease is poorly understood.[1] About 70% of the risk is believed to be genetic with many genes usually involved.[4] Other risk factors include a history of head injuries, depression, or hypertension.[1] The disease process is associated with plaques and tangles in the brain.[4] A probable diagnosis is based on the history of the illness and cognitive testing with medical imaging and blood tests to rule out other possible causes.[5] Initial symptoms are often mistaken for normal ageing.[1] Examination of brain tissue is needed for a definite diagnosis.[4]Mental and physical exercise, and avoiding obesity may decrease the risk of AD; however, evidence to support these recommendations is not strong.[4][12] There are no medications or supplements that have been shown to decrease risk.[13]
No treatments stop or reverse its progression, though some may temporarily improve symptoms.[2] Affected people increasingly rely on others for assistance, often placing a burden on the caregiver; the pressures can include social, psychological, physical, and economic elements.[14] Exercise programmes may be beneficial with respect to activities of daily living and can potentially improve outcomes.[15] Behavioural problems or psychosis due to dementia are often treated with antipsychotics, but this is not usually recommended, as there is little benefit with an increased risk of early death.[16][17]
In 2015, there were approximately 29.8 million people worldwide with AD.[2][8] It most often begins in people over 65 years of age, although 4% to 5% of cases are early-onset Alzheimer's which begin before this.[3] It affects about 6% of people 65 years and older.[1] In 2015, dementia resulted in about 1.9 million deaths.[9] It was first described by, and later named after, German psychiatrist and pathologist Alois Alzheimer in 1906.[18] In developed countries, AD is one of the most financially costly diseases.[19][20]
.mw-parser-output .toclimit-2 .toclevel-1 ul,.mw-parser-output .toclimit-3 .toclevel-2 ul,.mw-parser-output .toclimit-4 .toclevel-3 ul,.mw-parser-output .toclimit-5 .toclevel-4 ul,.mw-parser-output .toclimit-6 .toclevel-5 ul,.mw-parser-output .toclimit-7 .toclevel-6 ul{display:none}
Contents
1 Signs and symptoms
1.1 Pre-dementia
1.2 Early
1.3 Moderate
1.4 Advanced
2 Cause
2.1 Genetic
2.2 Cholinergic hypothesis
2.3 Amyloid hypothesis
2.4 Tau hypothesis
2.5 Other hypotheses
3 Pathophysiology
3.1 Neuropathology
3.2 Biochemistry
3.3 Disease mechanism
4 Diagnosis
4.1 Criteria
4.2 Techniques
5 Prevention
5.1 Medication
5.2 Lifestyle
5.3 Diet
6 Management
6.1 Medications
6.2 Psychosocial intervention
6.3 Caregiving
7 Prognosis
8 Epidemiology
9 History
10 Society and culture
10.1 Social costs
10.2 Caregiving burden
10.3 Media
11 Research directions
11.1 Drugs
11.2 Behavioral prevention
11.3 Possible transmission
11.4 Infections
11.5 Imaging
11.6 Early diagnosis
12 References
13 Further reading
14 External links
Signs and symptoms
.mw-parser-output .quotebox{background-color:#F9F9F9;border:1px solid #aaa;box-sizing:border-box;padding:10px;font-size:88%}.mw-parser-output .quotebox.floatleft{margin:0.5em 1.4em 0.8em 0}.mw-parser-output .quotebox.floatright{margin:0.5em 0 0.8em 1.4em}.mw-parser-output .quotebox.centered{margin:0.5em auto 0.8em auto}.mw-parser-output .quotebox.floatleft p,.mw-parser-output .quotebox.floatright p{font-style:inherit}.mw-parser-output .quotebox-title{background-color:#F9F9F9;text-align:center;font-size:larger;font-weight:bold}.mw-parser-output .quotebox-quote.quoted:before{font-family:"Times New Roman",serif;font-weight:bold;font-size:large;color:gray;content:" “ ";vertical-align:-45%;line-height:0}.mw-parser-output .quotebox-quote.quoted:after{font-family:"Times New Roman",serif;font-weight:bold;font-size:large;color:gray;content:" ” ";line-height:0}.mw-parser-output .quotebox .left-aligned{text-align:left}.mw-parser-output .quotebox .right-aligned{text-align:right}.mw-parser-output .quotebox .center-aligned{text-align:center}.mw-parser-output .quotebox cite{display:block;font-style:normal}@media screen and (max-width:360px){.mw-parser-output .quotebox{min-width:100%;margin:0 0 0.8em!important;float:none!important}}
Effects of ageing on memory but not AD
Forgetting things occasionally- Misplacing items sometimes
- Minor short-term memory loss
- Not remembering exact details
- Early stage Alzheimer's
- Not remembering episodes of forgetfulness
- Forgets names of family or friends
- Changes may only be noticed by close friends or relatives
- Some confusion in situations outside the familiar
- Middle stage Alzheimer's
- Greater difficulty remembering recently learned information
- Deepening confusion in many circumstances
- Problems with sleep
- Trouble determining their location
- Late stage Alzheimer's
- Poor ability to think
- Problems speaking
- Repeats same conversations
- More abusive, anxious, or paranoid
The disease course is divided into four stages, with a progressive pattern of cognitive and functional impairment.
Pre-dementia
The first symptoms are often mistakenly attributed to ageing or stress.[22] Detailed neuropsychological testing can reveal mild cognitive difficulties up to eight years before a person fulfils the clinical criteria for diagnosis of AD.[23] These early symptoms can affect the most complex activities of daily living.[24] The most noticeable deficit is short term memory loss, which shows up as difficulty in remembering recently learned facts and inability to acquire new information.[23][25]
Subtle problems with the executive functions of attentiveness, planning, flexibility, and abstract thinking, or impairments in semantic memory (memory of meanings, and concept relationships) can also be symptomatic of the early stages of AD.[23]Apathy can be observed at this stage, and remains the most persistent neuropsychiatric symptom throughout the course of the disease.[26] Depressive symptoms, irritability and reduced awareness of subtle memory difficulties are also common.[27]
The preclinical stage of the disease has also been termed mild cognitive impairment (MCI).[25] This is often found to be a transitional stage between normal ageing and dementia. MCI can present with a variety of symptoms, and when memory loss is the predominant symptom, it is termed "amnestic MCI" and is frequently seen as a prodromal stage of Alzheimer's disease.[28]
Early
In people with AD, the increasing impairment of learning and memory eventually leads to a definitive diagnosis. In a small percentage, difficulties with language, executive functions, perception (agnosia), or execution of movements (apraxia) are more prominent than memory problems.[29] AD does not affect all memory capacities equally. Older memories of the person's life (episodic memory), facts learned (semantic memory), and implicit memory (the memory of the body on how to do things, such as using a fork to eat or how to drink from a glass) are affected to a lesser degree than new facts or memories.[30][31]
Language problems are mainly characterised by a shrinking vocabulary and decreased word fluency, leading to a general impoverishment of oral and written language.[29][32] In this stage, the person with Alzheimer's is usually capable of communicating basic ideas adequately.[29][32][33] While performing fine motor tasks such as writing, drawing or dressing, certain movement coordination and planning difficulties (apraxia) may be present, but they are commonly unnoticed.[29] As the disease progresses, people with AD can often continue to perform many tasks independently, but may need assistance or supervision with the most cognitively demanding activities.[29]
Moderate
Progressive deterioration eventually hinders independence, with subjects being unable to perform most common activities of daily living.[29] Speech difficulties become evident due to an inability to recall vocabulary, which leads to frequent incorrect word substitutions (paraphasias). Reading and writing skills are also progressively lost.[29][33] Complex motor sequences become less coordinated as time passes and AD progresses, so the risk of falling increases.[29] During this phase, memory problems worsen, and the person may fail to recognise close relatives.[29]Long-term memory, which was previously intact, becomes impaired.[29]
Behavioural and neuropsychiatric changes become more prevalent. Common manifestations are wandering, irritability and labile affect, leading to crying, outbursts of unpremeditated aggression, or resistance to caregiving.[29]Sundowning can also appear.[34] Approximately 30% of people with AD develop illusionary misidentifications and other delusional symptoms.[29] Subjects also lose insight of their disease process and limitations (anosognosia).[29]Urinary incontinence can develop.[29] These symptoms create stress for relatives and carers, which can be reduced by moving the person from home care to other long-term care facilities.[29][35]
Advanced
During the final stages, the patient is completely dependent upon caregivers.[29] Language is reduced to simple phrases or even single words, eventually leading to complete loss of speech.[29][33] Despite the loss of verbal language abilities, people can often understand and return emotional signals. Although aggressiveness can still be present, extreme apathy and exhaustion are much more common symptoms. People with Alzheimer's disease will ultimately not be able to perform even the simplest tasks independently; muscle mass and mobility deteriorates to the point where they are bedridden and unable to feed themselves. The cause of death is usually an external factor, such as infection of pressure ulcers or pneumonia, not the disease itself.[29]
Cause
The cause for most Alzheimer's cases is still mostly unknown except for 1% to 5% of cases where genetic differences have been identified.[36][37] Several competing hypotheses exist trying to explain the cause of the disease.
Genetic
The genetic heritability of Alzheimer's disease (and memory components thereof), based on reviews of twin and family studies, ranges from 49% to 79%.[38][39] Around 0.1% of the cases are familial forms of autosomal (not sex-linked) dominant inheritance, which have an onset before age 65.[40] This form of the disease is known as early onset familial Alzheimer's disease. Most of autosomal dominant familial AD can be attributed to mutations in one of three genes: those encoding amyloid precursor protein (APP) and presenilins 1 and 2.[41] Most mutations in the APP and presenilin genes increase the production of a small protein called Aβ42, which is the main component of senile plaques.[42] Some of the mutations merely alter the ratio between Aβ42 and the other major forms—particularly Aβ40—without increasing Aβ42 levels.[43][44]
Most cases of Alzheimer's disease do not exhibit autosomal-dominant inheritance and are termed sporadic AD, in which environmental and genetic differences may act as risk factors. The best known genetic risk factor is the inheritance of the ε4 allele of the apolipoprotein E (APOE).[45][46] Between 40 and 80% of people with AD possess at least one APOEε4 allele.[46] The APOEε4 allele increases the risk of the disease by three times in heterozygotes and by 15 times in homozygotes.[40] Like many human diseases, environmental effects and genetic modifiers result in incomplete penetrance. For example, certain Nigerian populations do not show the relationship between dose of APOEε4 and incidence or age-of-onset for Alzheimer's disease seen in other human populations.[47][48] Early attempts to screen up to 400 candidate genes for association with late-onset sporadic AD (LOAD) resulted in a low yield.[40][41] More recent genome-wide association studies (GWAS) have found 19 areas in genes that appear to affect the risk.[49] These genes include: CASS4, CELF1, FERMT2, HLA-DRB5, INPP5D, MEF2C, NME8, PTK2B, SORL1, ZCWPW1, SlC24A4, CLU, PICALM, CR1, BIN1, MS4A, ABCA7, EPHA1, and CD2AP.[49]
Alleles in the TREM2 gene have been associated with a 3 to 5 times higher risk of developing Alzheimer's disease.[50][51] A suggested mechanism of action is that in some variants in TREM2 white blood cells in the brain are no longer able to control the amount of beta amyloid present. Many SNPs are associated with Alzheimer's with a 2018 study adding 30 SNPs by differentiating AD into 6 categories, including memory, language, visuospatial, and executive functioning.[52]
Cholinergic hypothesis
The oldest, on which most currently available drug therapies are based, is the cholinergic hypothesis,[53] which proposes that AD is caused by reduced synthesis of the neurotransmitter acetylcholine. The cholinergic hypothesis has not maintained widespread support, largely because medications intended to treat acetylcholine deficiency have not been very effective.[54]
Amyloid hypothesis
In 1991, the amyloid hypothesis postulated that extracellular amyloid beta (Aβ) deposits are the fundamental cause of the disease.[55][56] Support for this postulate comes from the location of the gene for the amyloid precursor protein (APP) on chromosome 21, together with the fact that people with trisomy 21 (Down Syndrome) who have an extra gene copy almost universally exhibit at least the earliest symptoms of AD by 40 years of age.[57][58] Also, a specific isoform of apolipoprotein, APOE4, is a major genetic risk factor for AD. While apolipoproteins enhance the breakdown of beta amyloid, some isoforms are not very effective at this task (such as APOE4), leading to excess amyloid buildup in the brain.[59] Further evidence comes from the finding that transgenic mice that express a mutant form of the human APP gene develop fibrillar amyloid plaques and Alzheimer's-like brain pathology with spatial learning deficits.[60]
An experimental vaccine was found to clear the amyloid plaques in early human trials, but it did not have any significant effect on dementia.[61] Researchers have been led to suspect non-plaque Aβoligomers (aggregates of many monomers) as the primary pathogenic form of Aβ. These toxic oligomers, also referred to as amyloid-derived diffusible ligands (ADDLs), bind to a surface receptor on neurons and change the structure of the synapse, thereby disrupting neuronal communication.[62] One receptor for Aβ oligomers may be the prion protein, the same protein that has been linked to mad cow disease and the related human condition, Creutzfeldt–Jakob disease, thus potentially linking the underlying mechanism of these neurodegenerative disorders with that of Alzheimer's disease.[63]
In 2009, this theory was updated, suggesting that a close relative of the beta-amyloid protein, and not necessarily the beta-amyloid itself, may be a major culprit in the disease. The theory holds that an amyloid-related mechanism that prunes neuronal connections in the brain in the fast-growth phase of early life may be triggered by ageing-related processes in later life to cause the neuronal withering of Alzheimer's disease.[64] N-APP, a fragment of APP from the peptide's N-terminus, is adjacent to beta-amyloid and is cleaved from APP by one of the same enzymes. N-APP triggers the self-destruct pathway by binding to a neuronal receptor called death receptor 6 (DR6, also known as TNFRSF21).[64] DR6 is highly expressed in the human brain regions most affected by Alzheimer's, so it is possible that the N-APP/DR6 pathway might be hijacked in the ageing brain to cause damage. In this model, beta-amyloid plays a complementary role, by depressing synaptic function.
In early 2017, a trial of verubecestat, which inhibits the beta-secretase protein responsible for creating beta-amyloid protein was discontinued as an independent panel found "virtually no chance of finding a positive clinical effect".[65]
Tau hypothesis

In Alzheimer's disease, changes in tau protein lead to the disintegration of microtubules in brain cells.
The tau hypothesis proposes that tau protein abnormalities initiate the disease cascade.[56] In this model, hyperphosphorylated tau begins to pair with other threads of tau. Eventually, they form neurofibrillary tangles inside nerve cell bodies.[66] When this occurs, the microtubules disintegrate, destroying the structure of the cell's cytoskeleton which collapses the neuron's transport system.[67] This may result first in malfunctions in biochemical communication between neurons and later in the death of the cells.[68]
Other hypotheses
A neurovascular hypothesis has been proposed which states that poor functioning of the blood–brain barrier may be involved.[69]
The cellular homeostasis of biometals such as ionic copper, iron, and zinc is disrupted in AD, though it remains unclear whether this is produced by or causes the changes in proteins. These ions affect and are affected by tau, APP, and APOE,[70] and their dysregulation may cause oxidative stress that may contribute to the pathology.[71][72][73][74][75] The quality of some of these studies has been criticised,[76][77] and the link remains controversial.[78] The majority of researchers do not support a causal connection with aluminium.[77]
Smoking is a significant AD risk factor.[79]Systemic markers of the innate immune system are risk factors for late-onset AD.[80]
There is tentative evidence that exposure to air pollution may be a contributing factor to the development of Alzheimer's disease.[81]
Gum disease: An infection with Spirochetes (a bacterium) in gum disease may cause dementia and may be involved in the pathogenesis of Alzheimer's disease.[82] A fungal infection may also be a factor.[83]
One hypothesis posits that dysfunction of oligodendrocytes and their associated myelin during aging contributes to axon damage, which then causes amyloid production and tau hyper-phosphorylation as a side effect.[84][85]
Retrogenesis is a medical hypothesis about the development and progress of Alzheimer's disease proposed by Barry Reisberg in the 1980s.[86] The hypothesis is that just as the fetus goes through a process of neurodevelopment beginning with neurulation and ending with myelination, the brains of people with AD go through a reverse neurodegeneration process starting with demyelination and death of axons (white matter) and ending with the death of grey matter.[87] Likewise the hypothesis is, that as infants go through states of cognitive development, people with AD go through the reverse process of progressive cognitive impairment.[86] Reisberg developed the caregiving assessment tool known as "FAST" (Functional Assessment Staging Tool) which he says allows those caring for AD patients to identify the stages of disease progression and that provides advice about the kind of care needed at each stage.[86][88]
Pathophysiology

Histopathologic image of senile plaques seen in the cerebral cortex of a person with Alzheimer's disease of presenile onset. Silver impregnation.

There is cortical atrophy in Alzheimer's disease, associated with loss of gyri and sulci in the temporal lobe and parietal lobe, and parts of the frontal cortex and cingulate gyrus.
Neuropathology
Alzheimer's disease is characterised by loss of neurons and synapses in the cerebral cortex and certain subcortical regions. This loss results in gross atrophy of the affected regions, including degeneration in the temporal lobe and parietal lobe, and parts of the frontal cortex and cingulate gyrus.[89] Degeneration is also present in brainstem nuclei like the locus coeruleus.[90] Studies using MRI and PET have documented reductions in the size of specific brain regions in people with AD as they progressed from mild cognitive impairment to Alzheimer's disease, and in comparison with similar images from healthy older adults.[91][92]
Both amyloid plaques and neurofibrillary tangles are clearly visible by microscopy in brains of those afflicted by AD.[93] Plaques are dense, mostly insoluble deposits of beta-amyloid peptide and cellular material outside and around neurons. Tangles (neurofibrillary tangles) are aggregates of the microtubule-associated protein tau which has become hyperphosphorylated and accumulate inside the cells themselves. Although many older individuals develop some plaques and tangles as a consequence of ageing, the brains of people with AD have a greater number of them in specific brain regions such as the temporal lobe.[94]Lewy bodies are not rare in the brains of people with AD.[95]
Biochemistry
@media all and (max-width:720px){.mw-parser-output .tmulti>.thumbinner{width:100%!important;max-width:none!important}.mw-parser-output .tmulti .tsingle{float:none!important;max-width:none!important;width:100%!important;text-align:center}}
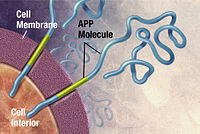


Alzheimer's disease has been identified as a protein misfolding disease (proteopathy), caused by plaque accumulation of abnormally folded amyloid beta protein and tau protein in the brain.[96] Plaques are made up of small peptides, 39–43 amino acids in length, called amyloid beta (Aβ). Aβ is a fragment from the larger amyloid precursor protein (APP). APP is a transmembrane protein that penetrates through the neuron's membrane. APP is critical to neuron growth, survival, and post-injury repair.[97][98] In Alzheimer's disease, gamma secretase and beta secretase act together in a proteolytic process which causes APP to be divided into smaller fragments.[99] One of these fragments gives rise to fibrils of amyloid beta, which then form clumps that deposit outside neurons in dense formations known as senile plaques.[93][100]
AD is also considered a tauopathy due to abnormal aggregation of the tau protein. Every neuron has a cytoskeleton, an internal support structure partly made up of structures called microtubules. These microtubules act like tracks, guiding nutrients and molecules from the body of the cell to the ends of the axon and back. A protein called tau stabilises the microtubules when phosphorylated, and is therefore called a microtubule-associated protein. In AD, tau undergoes chemical changes, becoming hyperphosphorylated; it then begins to pair with other threads, creating neurofibrillary tangles and disintegrating the neuron's transport system.[101] Pathogenic tau can also cause neuronal death through transposable element dysregulation.[102]
Disease mechanism
Exactly how disturbances of production and aggregation of the beta-amyloid peptide give rise to the pathology of AD is not known.[103][104]
The amyloid hypothesis traditionally points to the accumulation of beta-amyloid peptides as the central event triggering neuron degeneration. Accumulation of aggregated amyloid fibrils, which are believed to be the toxic form of the protein responsible for disrupting the cell's calcium ion homeostasis, induces programmed cell death (apoptosis).[105] It is also known that Aβ selectively builds up in the mitochondria in the cells of Alzheimer's-affected brains, and it also inhibits certain enzyme functions and the utilisation of glucose by neurons.[106]
Various inflammatory processes and cytokines may also have a role in the pathology of Alzheimer's disease. Inflammation is a general marker of tissue damage in any disease, and may be either secondary to tissue damage in AD or a marker of an immunological response.[107] There is increasing evidence of a strong interaction between the neurons and the immunological mechanisms in the brain. Obesity and systemic inflammation may interfere with immunological processes which promote disease progression.[108]
Alterations in the distribution of different neurotrophic factors and in the expression of their receptors such as the brain-derived neurotrophic factor (BDNF) have been described in AD.[109][110]
Diagnosis

PET scan of the brain of a person with AD showing a loss of function in the temporal lobe
Alzheimer's disease is usually diagnosed based on the person's medical history, history from relatives, and behavioural observations. The presence of characteristic neurological and neuropsychological features and the absence of alternative conditions is supportive.[111][112] Advanced medical imaging with computed tomography (CT) or magnetic resonance imaging (MRI), and with single-photon emission computed tomography (SPECT) or positron emission tomography (PET) can be used to help exclude other cerebral pathology or subtypes of dementia.[113] Moreover, it may predict conversion from prodromal stages (mild cognitive impairment) to Alzheimer's disease.[114]
Assessment of intellectual functioning including memory testing can further characterise the state of the disease.[22] Medical organisations have created diagnostic criteria to ease and standardise the diagnostic process for practising physicians. The diagnosis can be confirmed with very high accuracy post-mortem when brain material is available and can be examined histologically.[115]
Criteria
The National Institute of Neurological and Communicative Disorders and Stroke (NINCDS) and the Alzheimer's Disease and Related Disorders Association (ADRDA, now known as the Alzheimer's Association) established the most commonly used NINCDS-ADRDA Alzheimer's Criteria for diagnosis in 1984,[115] extensively updated in 2007.[116] These criteria require that the presence of cognitive impairment, and a suspected dementia syndrome, be confirmed by neuropsychological testing for a clinical diagnosis of possible or probable AD. A histopathologic confirmation including a microscopic examination of brain tissue is required for a definitive diagnosis. Good statistical reliability and validity have been shown between the diagnostic criteria and definitive histopathological confirmation.[117] Eight intellectual domains are most commonly impaired in AD—memory, language, perceptual skills, attention, motor skills, orientation, problem solving and executive functional abilities. These domains are equivalent to the NINCDS-ADRDA Alzheimer's Criteria as listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) published by the American Psychiatric Association.[118][119]
Techniques

Neuropsychological screening tests can help in the diagnosis of AD. In the tests, people are instructed to copy drawings similar to the one shown in the picture, remember words, read, and subtract serial numbers.
Neuropsychological tests such as the mini–mental state examination (MMSE) are widely used to evaluate the cognitive impairments needed for diagnosis. More comprehensive test arrays are necessary for high reliability of results, particularly in the earliest stages of the disease.[120][121]Neurological examination in early AD will usually provide normal results, except for obvious cognitive impairment, which may not differ from that resulting from other diseases processes, including other causes of dementia.
Further neurological examinations are crucial in the differential diagnosis of AD and other diseases.[22] Interviews with family members are also utilised in the assessment of the disease. Caregivers can supply important information on the daily living abilities, as well as on the decrease, over time, of the person's mental function.[122] A caregiver's viewpoint is particularly important, since a person with AD is commonly unaware of his own deficits.[123] Many times, families also have difficulties in the detection of initial dementia symptoms and may not communicate accurate information to a physician.[124]
Supplemental testing provides extra information on some features of the disease or is used to rule out other diagnoses. Blood tests can identify other causes for dementia than AD[22]—causes which may, in rare cases, be reversible.[125] It is common to perform thyroid function tests, assess B12, rule out syphilis, rule out metabolic problems (including tests for kidney function, electrolyte levels and for diabetes), assess levels of heavy metals (e.g. lead, mercury) and anaemia. (It is also necessary to rule out delirium).
Psychological tests for depression are employed, since depression can either be concurrent with AD (see Depression of Alzheimer disease), an early sign of cognitive impairment,[126] or even the cause.[127][128]
Due to low accuracy, the C-PIB-PET scan is not recommended to be used as an early diagnostic tool or for predicting the development of Alzheimer's disease when people show signs of mild cognitive impairment (MCI).[129] The use of ¹⁸F-FDG PET scans, as a single test, to identify people who may develop Alzheimer's disease is also not supported by evidence.[130]
Prevention
Intellectual activities such as playing chess or regular social interaction have been linked to a reduced risk of AD in epidemiological studies, although no causal relationship has been found.
There is no definitive evidence to support that any particular measure is effective in preventing AD.[13] Global studies of measures to prevent or delay the onset of AD have often produced inconsistent results.
Epidemiological studies have proposed relationships between certain modifiable factors, such as diet, cardiovascular risk, pharmaceutical products, or intellectual activities among others, and a population's likelihood of developing AD. Only further research, including clinical trials, will reveal whether these factors can help to prevent AD.[13]
Medication
Although cardiovascular risk factors, such as hypercholesterolaemia, hypertension, diabetes, and smoking, are associated with a higher risk of onset and course of AD,[131][132]statins, which are cholesterol lowering drugs, have not been effective in preventing or improving the course of the disease.[133][134][135]
Long-term usage of non-steroidal anti-inflammatory drugs (NSAIDs) were thought in 2007 to be associated with a reduced likelihood of developing AD.[136] Evidence also suggested the notion that NSAIDs could reduce inflammation related to amyloid plaques, but trials were suspended due to high adverse events.[13] No prevention trial has been completed.[13] They do not appear to be useful as a treatment, but as of 2011[update] were thought to be candidates as presymptomatic preventatives.[137]Hormone replacement therapy in menopause, although previously used, may increase the risk of dementia.[138]
Lifestyle
People who engage in intellectual activities such as reading, playing board games, completing crossword puzzles, playing musical instruments, or regular social interaction show a reduced risk for Alzheimer's disease.[139] This is compatible with the cognitive reserve theory, which states that some life experiences result in more efficient neural functioning providing the individual a cognitive reserve that delays the onset of dementia manifestations.[139]Education delays the onset of AD syndrome without changing the duration of the disease.[140] Learning a second language even later in life seems to delay getting Alzheimer disease.[141]Physical activity is also associated with a reduced risk of AD.[140] Physical exercise is associated with decreased rate of dementia.[142] Physical exercise is also effective in reducing symptom severity in those with Alzheimers.[143]
Diet
People who maintain a healthy, Japanese, or Mediterranean diet have a reduced risk of AD.[144] A Mediterranean diet may improve outcomes in those with the disease.[145] Those who eat a diet high in saturated fats and simple carbohydrates (mono- and disaccharide) have a higher risk.[146] The Mediterranean diet's beneficial cardiovascular effect has been proposed as the mechanism of action.[147]
Conclusions on dietary components have at times been difficult to ascertain as results have differed between population-based studies and randomised controlled trials.[144] There is limited evidence that light to moderate use of alcohol, particularly red wine, is associated with lower risk of AD.[144] There is tentative evidence that caffeine may be protective.[148] A number of foods high in flavonoids such as cocoa, red wine, and tea may decrease the risk of AD.[149][150]
Reviews on the use of vitamins and minerals have not found enough consistent evidence to recommend them. This includes vitamin A,[151][152] C,[153][154] the alpha-tocopherol form of vitamin E,[155]selenium,[156]zinc,[157][158] and folic acid with or without vitamin B12.[159] Evidence from one randomized controlled trial indicated that the alpha-tocopherol form of vitamin E may slow cognitive decline, this evidence was judged to be "moderate" in quality.[155] Trials examining folic acid (B9) and other B vitamins failed to show any significant association with cognitive decline.[160] Omega-3 fatty acid supplements from plants and fish, and dietary docosahexaenoic acid (DHA), do not appear to benefit people with mild to moderate Alzheimer's disease.[161][162]
Curcumin as of 2010[update] had not shown benefit in people even though there is tentative evidence in animals.[163] There was inconsistent and unconvincing evidence that ginkgo has any positive effect on cognitive impairment and dementia.[164] As of 2008[update] there was no concrete evidence that cannabinoids are effective in improving the symptoms of AD or dementia;[165] however, some research into endocannabinoids looked promising.[166]
Management
There is no cure for Alzheimer's disease; available treatments offer relatively small symptomatic benefit but remain palliative in nature. Current treatments can be divided into pharmaceutical, psychosocial and caregiving.
Medications

Three-dimensional molecular model of donepezil, an acetylcholinesterase inhibitor used in the treatment of AD symptoms

Molecular structure of memantine, a medication approved for advanced AD symptoms
Five medications are currently used to treat the cognitive problems of AD: four are acetylcholinesterase inhibitors (tacrine, rivastigmine, galantamine and donepezil) and the other (memantine) is an NMDA receptor antagonist. The benefit from their use is small.[6][167][168] No medication has been clearly shown to delay or halt the progression of the disease.
Reduction in the activity of the cholinergic neurons is a well-known feature of Alzheimer's disease.[169] Acetylcholinesterase inhibitors are employed to reduce the rate at which acetylcholine (ACh) is broken down, thereby increasing the concentration of ACh in the brain and combating the loss of ACh caused by the death of cholinergic neurons.[170] There is evidence for the efficacy of these medications in mild to moderate Alzheimer's disease,[171][168][167] and some evidence for their use in the advanced stage.[167] The use of these drugs in mild cognitive impairment has not shown any effect in a delay of the onset of AD.[172] The most common side effects are nausea and vomiting, both of which are linked to cholinergic excess. These side effects arise in approximately 10–20% of users, are mild to moderate in severity, and can be managed by slowly adjusting medication doses.[173] Less common secondary effects include muscle cramps, decreased heart rate (bradycardia), decreased appetite and weight, and increased gastric acid production.[171]
Glutamate is an excitatory neurotransmitter of the nervous system, although excessive amounts in the brain can lead to cell death through a process called excitotoxicity which consists of the overstimulation of glutamate receptors. Excitotoxicity occurs not only in Alzheimer's disease, but also in other neurological diseases such as Parkinson's disease and multiple sclerosis.[174]Memantine is a noncompetitive NMDA receptor antagonist first used as an anti-influenza agent. It acts on the glutamatergic system by blocking NMDA receptors and inhibiting their overstimulation by glutamate.[174][175] Memantine has been shown to have a small benefit in the treatment of Alzheimer's disease.[176] Reported adverse events with memantine are infrequent and mild, including hallucinations, confusion, dizziness, headache and fatigue.[177] The combination of memantine and donepezil has been shown to be "of statistically significant but clinically marginal effectiveness".[178]
Atypical antipsychotics are modestly useful in reducing aggression and psychosis in people with Alzheimer's disease, but their advantages are offset by serious adverse effects, such as stroke, movement difficulties or cognitive decline.[179] When used in the long-term, they have been shown to associate with increased mortality.[180] Stopping antipsychotic use in this group of people appears to be safe.[181]
Huperzine A while promising, requires further evidence before its use can be recommended.[182]
Psychosocial intervention
Psychosocial interventions are used as an adjunct to pharmaceutical treatment and can be classified within behaviour-, emotion-, cognition- or stimulation-oriented approaches. Research on efficacy is unavailable and rarely specific to AD, focusing instead on dementia in general.[183]
Behavioural interventions attempt to identify and reduce the antecedents and consequences of problem behaviours. This approach has not shown success in improving overall functioning,[184] but can help to reduce some specific problem behaviours, such as incontinence.[185] There is a lack of high quality data on the effectiveness of these techniques in other behaviour problems such as wandering.[186][187] Music therapy is effective in reducing behavioural and psychological symptoms.[188]
Emotion-oriented interventions include reminiscence therapy, validation therapy, supportive psychotherapy, sensory integration, also called snoezelen, and simulated presence therapy. A Cochrane review has found no evidence that this is effective.[189] Supportive psychotherapy has received little or no formal scientific study, but some clinicians find it useful in helping mildly impaired people adjust to their illness.[183] Reminiscence therapy (RT) involves the discussion of past experiences individually or in group, many times with the aid of photographs, household items, music and sound recordings, or other familiar items from the past. A 2018 review of the effectiveness of RT found that effects were inconsistent, small in size and of doubtful clinical significance, and varied by setting.[190] Simulated presence therapy (SPT) is based on attachment theories and involves playing a recording with voices of the closest relatives of the person with Alzheimer's disease. There is partial evidence indicating that SPT may reduce challenging behaviours.[191]
Finally, validation therapy is based on acceptance of the reality and personal truth of another's experience, while sensory integration is based on exercises aimed to stimulate senses. There is no evidence to support the usefulness of these therapies.[192][193]
The aim of cognition-oriented treatments, which include reality orientation and cognitive retraining, is the reduction of cognitive deficits. Reality orientation consists in the presentation of information about time, place or person to ease the understanding of the person about its surroundings and his or her place in them. On the other hand, cognitive retraining tries to improve impaired capacities by exercitation of mental abilities. Both have shown some efficacy improving cognitive capacities,[194][195] although in some studies these effects were transient and negative effects, such as frustration, have also been reported.[183]
Stimulation-oriented treatments include art, music and pet therapies, exercise, and any other kind of recreational activities. Stimulation has modest support for improving behaviour, mood, and, to a lesser extent, function. Nevertheless, as important as these effects are, the main support for the use of stimulation therapies is the change in the person's routine.[183] The efficacy of non-invasive brain stimulation and invasive brain stimulation in AD remains uncertain.[196]
Caregiving
Since Alzheimer's has no cure and it gradually renders people incapable of tending for their own needs, caregiving is essentially the treatment and must be carefully managed over the course of the disease.
During the early and moderate stages, modifications to the living environment and lifestyle can increase patient safety and reduce caretaker burden.[197][198] Examples of such modifications are the adherence to simplified routines, the placing of safety locks, the labelling of household items to cue the person with the disease or the use of modified daily life objects.[183][199][200] If eating becomes problematic, food will need to be prepared in smaller pieces or even pureed.[201] When swallowing difficulties arise, the use of feeding tubes may be required. In such cases, the medical efficacy and ethics of continuing feeding is an important consideration of the caregivers and family members.[202][203] The use of physical restraints is rarely indicated in any stage of the disease, although there are situations when they are necessary to prevent harm to the person with AD or their caregivers.[183]
As the disease progresses, different medical issues can appear, such as oral and dental disease, pressure ulcers, malnutrition, hygiene problems, or respiratory, skin, or eye infections. Careful management can prevent them, while professional treatment is needed when they do arise.[204][205] During the final stages of the disease, treatment is centred on relieving discomfort until death, often with the help of hospice.[206]
Prognosis

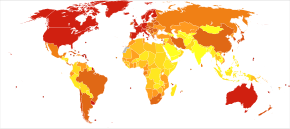
Disability-adjusted life year for Alzheimer and other dementias per 100,000 inhabitants in 2004. .mw-parser-output .refbegin{font-size:90%;margin-bottom:0.5em}.mw-parser-output .refbegin-hanging-indents>ul{list-style-type:none;margin-left:0}.mw-parser-output .refbegin-hanging-indents>ul>li,.mw-parser-output .refbegin-hanging-indents>dl>dd{margin-left:0;padding-left:3.2em;text-indent:-3.2em;list-style:none}.mw-parser-output .refbegin-100{font-size:100%}
No data
≤ 50
50–70
70–90
90–110
110–130
130–150
150–170
170–190
190–210
210–230
230–250
≥ 250
The early stages of Alzheimer's disease are difficult to diagnose. A definitive diagnosis is usually made once cognitive impairment compromises daily living activities, although the person may still be living independently. The symptoms will progress from mild cognitive problems, such as memory loss through increasing stages of cognitive and non-cognitive disturbances, eliminating any possibility of independent living, especially in the late stages of the disease.[29]
Life expectancy of people with AD is reduced.[207] Following diagnosis it typically ranges from three to ten years.[207]
Fewer than 3% of people live more than fourteen years.[208] Disease features significantly associated with reduced survival are an increased severity of cognitive impairment, decreased functional level, history of falls, and disturbances in the neurological examination. Other coincident diseases such as heart problems, diabetes or history of alcohol abuse are also related with shortened survival.[209][210][211] While the earlier the age at onset the higher the total survival years, life expectancy is particularly reduced when compared to the healthy population among those who are younger.[212] Men have a less favourable survival prognosis than women.[208][213]
Pneumonia and dehydration are the most frequent immediate causes of death brought by AD, while cancer is a less frequent cause of death than in the general population.[213]
Epidemiology
| Age | New affected per thousand person–years |
|---|---|
| 65–69 | 3 |
| 70–74 | 6 |
| 75–79 | 9 |
| 80–84 | 23 |
| 85–89 | 40 |
| 90– | 69 |
Two main measures are used in epidemiological studies: incidence and prevalence. Incidence is the number of new cases per unit of person–time at risk (usually number of new cases per thousand person–years); while prevalence is the total number of cases of the disease in the population at any given time.
Regarding incidence, cohort longitudinal studies (studies where a disease-free population is followed over the years) provide rates between 10 and 15 per thousand person–years for all dementias and 5–8 for AD,[214][215] which means that half of new dementia cases each year are AD. Advancing age is a primary risk factor for the disease and incidence rates are not equal for all ages: every five years after the age of 65, the risk of acquiring the disease approximately doubles, increasing from 3 to as much as 69 per thousand person years.[214][215] There are also sex differences in the incidence rates, women having a higher risk of developing AD particularly in the population older than 85.[215][216] In the United States, the risk of dying from Alzheimer's disease is 26% higher among the non-Hispanic white population than among the non-Hispanic black population, whereas the Hispanic population has a 30% lower risk than the non-Hispanic white population.[217]
Deaths per million persons in 2012 due to dementias including Alzheimer's disease
0–4
5–8
9–10
11–13
14–17
18–24
25–45
46–114
115–375
376–1266
Prevalence of AD in populations is dependent upon different factors including incidence and survival. Since the incidence of AD increases with age, it is particularly important to include the mean age of the population of interest. In the United States, Alzheimer prevalence was estimated to be 1.6% in 2000 both overall and in the 65–74 age group, with the rate increasing to 19% in the 75–84 group and to 42% in the greater than 84 group.[218] Prevalence rates in less developed regions are lower.[219] The World Health Organization estimated that in 2005, 0.379% of people worldwide had dementia, and that the prevalence would increase to 0.441% in 2015 and to 0.556% in 2030.[220] Other studies have reached similar conclusions.[219] Another study estimated that in 2006, 0.40% of the world population (range 0.17–0.89%; absolute number 26.6 million, range 11.4–59.4 million) were afflicted by AD, and that the prevalence rate would triple and the absolute number would quadruple by 2050.[221]
History

Alois Alzheimer's patient Auguste Deter in 1902. Hers was the first described case of what became known as Alzheimer's disease.
The ancient Greek and Roman philosophers and physicians associated old age with increasing dementia.[18] It was not until 1901 that German psychiatrist Alois Alzheimer identified the first case of what became known as Alzheimer's disease, named after him, in a fifty-year-old woman he called Auguste D. He followed her case until she died in 1906, when he first reported publicly on it.[222] During the next five years, eleven similar cases were reported in the medical literature, some of them already using the term Alzheimer's disease.[18] The disease was first described as a distinctive disease by Emil Kraepelin after suppressing some of the clinical (delusions and hallucinations) and pathological features (arteriosclerotic changes) contained in the original report of Auguste D.[223] He included Alzheimer's disease, also named presenile dementia by Kraepelin, as a subtype of senile dementia in the eighth edition of his Textbook of Psychiatry, published on 15 July, 1910.[224]
For most of the 20th century, the diagnosis of Alzheimer's disease was reserved for individuals between the ages of 45 and 65 who developed symptoms of dementia. The terminology changed after 1977 when a conference on AD concluded that the clinical and pathological manifestations of presenile and senile dementia were almost identical, although the authors also added that this did not rule out the possibility that they had different causes.[225] This eventually led to the diagnosis of Alzheimer's disease independent of age.[226] The term senile dementia of the Alzheimer type (SDAT) was used for a time to describe the condition in those over 65, with classical Alzheimer's disease being used to describe those who were younger. Eventually, the term Alzheimer's disease was formally adopted in medical nomenclature to describe individuals of all ages with a characteristic common symptom pattern, disease course, and neuropathology.[227]
Society and culture
Social costs
Dementia, and specifically Alzheimer's disease, may be among the most costly diseases for society in Europe and the United States,[19][20] while their costs in other countries such as Argentina,[228] and South Korea,[229] are also high and rising. These costs will probably increase with the ageing of society, becoming an important social problem. AD-associated costs include direct medical costs such as nursing home care, direct nonmedical costs such as in-home day care, and indirect costs such as lost productivity of both patient and caregiver.[20] Numbers vary between studies but dementia costs worldwide have been calculated around $160 billion,[230] while costs of Alzheimer's disease in the United States may be $100 billion each year.[20]
The greatest origin of costs for society is the long-term care by health care professionals and particularly institutionalisation, which corresponds to 2/3 of the total costs for society.[19]The cost of living at home is also very high,[19] especially when informal costs for the family, such as caregiving time and caregiver's lost earnings, are taken into account.[231]
Costs increase with dementia severity and the presence of behavioural disturbances,[232] and are related to the increased caregiving time required for the provision of physical care.[231] Therefore, any treatment that slows cognitive decline, delays institutionalisation or reduces caregivers' hours will have economic benefits. Economic evaluations of current treatments have shown positive results.[20]
Caregiving burden
The role of the main caregiver is often taken by the spouse or a close relative.[233] Alzheimer's disease is known for placing a great burden on caregivers which includes social, psychological, physical or economic aspects.[14][234][235] Home care is usually preferred by people with AD and their families.[236] This option also delays or eliminates the need for more professional and costly levels of care.[236][237] Nevertheless, two-thirds of nursing home residents have dementias.[183]
Dementia caregivers are subject to high rates of physical and mental disorders.[238] Factors associated with greater psychosocial problems of the primary caregivers include having an affected person at home, the carer being a spouse, demanding behaviours of the cared person such as depression, behavioural disturbances, hallucinations, sleep problems or walking disruptions and social isolation.[239][240] Regarding economic problems, family caregivers often give up time from work to spend 47 hours per week on average with the person with AD, while the costs of caring for them are high. Direct and indirect costs of caring for an Alzheimer's patient average between $18,000 and $77,500 per year in the United States, depending on the study.[231][233]
Cognitive behavioural therapy and the teaching of coping strategies either individually or in group have demonstrated their efficacy in improving caregivers' psychological health.[14][241]
Media
AD has been portrayed in films such as: Iris (2001), based on John Bayley's memoir of his wife Iris Murdoch;[242]The Notebook (2004), based on Nicholas Sparks' 1996 novel of the same name;[243]A Moment to Remember (2004);Thanmathra (2005);[244]Memories of Tomorrow (Ashita no Kioku) (2006), based on Hiroshi Ogiwara's novel of the same name;[245]Away from Her (2006), based on Alice Munro's short story "The Bear Came over the Mountain";[246]Still Alice (2014), about a Columbia University professor who has early onset Alzheimer's disease, based on Lisa Genova's 2007 novel of the same name and featuring Julianne Moore in the title role. Documentaries on Alzheimer's disease include Malcolm and Barbara: A Love Story (1999) and Malcolm and Barbara: Love's Farewell (2007), both featuring Malcolm Pointon.[247][248][249]
Research directions
Drugs
In the decade 2002–2012, 244 compounds were assessed in Phase I, Phase II, or Phase III trials, and only one of these (memantine) received FDA approval (though others were still in the pipeline).[250]Solanezumab failed to show effectiveness in patients who already had Alzheimer's symptoms.
One area of clinical research is focused on treating the underlying disease pathology. Reduction of beta-amyloid levels is a common target of compounds[251] (such as apomorphine) under investigation. Immunotherapy or vaccination for the amyloid protein is one treatment modality under study.[252] Unlike preventative vaccination, the putative therapy would be used to treat people already diagnosed. It is based upon the concept of training the immune system to recognise, attack, and reverse deposition of amyloid, thereby altering the course of the disease.[253] An example of such a vaccine under investigation was ACC-001,[254][255] although the trials were suspended in 2008.[256] Another similar agent is bapineuzumab, an antibody designed as identical to the naturally induced anti-amyloid antibody.[257] However, immunotherapeutic agents have been found to cause some concerning adverse drug reactions, such as amyloid-related imaging abnormalities.[258] Other approaches are neuroprotective agents, such as AL-108,[259] and metal-protein interaction attenuation agents, such as PBT2.[260] A TNFα receptor-blocking fusion protein, etanercept has showed encouraging results.[261]
In 2008, two separate clinical trials showed positive results in modifying the course of disease in mild to moderate AD with methylthioninium chloride, a drug that inhibits tau aggregation,[262][263] and dimebon, an antihistamine.[264]
The consecutive phase-III trial of dimebon failed to show positive effects in the primary and secondary endpoints.[265][266][267] Work with methylthioninium chloride showed that bioavailability of methylthioninium from the gut was affected by feeding and by stomach acidity, leading to unexpectedly variable dosing.[268] A new stabilised formulation, as the prodrug LMTX, is in phase-III trials (in 2014).[269]
Behavioral prevention
Preliminary research on the effects of meditation on retrieving memory and cognitive functions have been encouraging.[270][qualify evidence] A 2015 review suggests that mindfulness-based interventions may prevent or delay the onset of mild cognitive impairment and Alzheimer's disease.[271]
Possible transmission
Rare cases of possible transmission between people are being studied,[272] e.g. to growth hormone patients.[273]
Infections
The herpes simplex virus HSV-1 has been found in the same areas as amyloid plaques.[274] This suggested the possibility that AD could be treated or prevented with antiviral medication.[274][275] Studies of antivirals in cell cultures have shown promising results.[276]
Fungal infection of AD brain has also been described.[277]
This hypothesis was proposed by the microbiologist L. Carrasco when his group found statistical correlation between disseminated mycoses and AD.[278]
Further work revealed that fungal infection is present in different brain regions of AD patients, but not in the control individuals.[279][280]
A fungal infection explains the symptoms observed in AD patients. The slow progression of AD fits with the chronic nature of some systemic fungal infections, which can be asymptomatic and thus, unnoticed and untreated.[279]
The fungal hypotheses are also compatible with some other established AD hypotheses, like the amyloid hypothesis, that can be explained as an immune system response to an infection in the CNS,[281][282][283] as found by R. Moir and R. Tanzi in mouse and worm models of AD.
Imaging
Of the many medical imaging techniques available, single photon emission computed tomography (SPECT) appears to be superior in differentiating Alzheimer's disease from other types of dementia, and this has been shown to give a greater level of accuracy compared with mental testing and medical history analysis.[284] Advances have led to the proposal of new diagnostic criteria.[22][116]
PiB PET remains investigational, but a similar PET scanning radiopharmaceutical called florbetapir, containing the longer-lasting radionuclide fluorine-18, is a diagnostic tool in Alzheimer's disease.[285][286]
Amyloid imaging is likely to be used in conjunction with other markers rather than as an alternative.[287] Volumetric MRI can detect changes in the size of brain regions. Measuring those regions that atrophy during the progress of Alzheimer's disease is showing promise as a diagnostic indicator. It may prove less expensive than other imaging methods currently under study.[288]
In 2011 An FDA panel voted unanimously to recommend approval of florbetapir. The imaging agent can help to detect Alzheimer's brain plaques.[289] A negative scan indicates sparse or no plaques, which is not consistent with a diagnosis of AD.[290]
Early diagnosis
Emphasis in Alzheimer's research has been placed on diagnosing the condition before symptoms begin.[291] A number of biochemical tests have been developed to enable earlier detection. Some such tests involve the analysis of cerebrospinal fluid for beta-amyloid, total tau protein and phosphorylated tau181P protein concentrations.[292] Because drawing CSF can be painful, repeated draws are avoided. A blood test for circulatory miRNA and inflammatory biomarkers is a potential alternative indicator.[292]
References
^ abcdefghijklm Burns A, Iliffe S (February 2009). "Alzheimer's disease". BMJ. 338: b158. doi:10.1136/bmj.b158. PMID 19196745.
^ abcdefgh "Dementia Fact sheet". World Health Organization. 12 December 2017.
^ ab Mendez MF (November 2012). "Early-onset Alzheimer's disease: nonamnestic subtypes and type 2 AD". Archives of Medical Research. 43 (8): 677–85. doi:10.1016/j.arcmed.2012.11.009. PMC 3532551. PMID 23178565.
^ abcde Ballard C, Gauthier S, Corbett A, Brayne C, Aarsland D, Jones E (March 2011). "Alzheimer's disease". Lancet. 377 (9770): 1019–31. doi:10.1016/S0140-6736(10)61349-9. PMID 21371747.
^ ab "Dementia diagnosis and assessment" (PDF). National Institute for Health and Care Excellence (NICE). Archived from the original (PDF) on 5 December 2014. Retrieved 30 November 2014.
^ ab Commission de la transparence. Médicaments de la maladie d'Alzheimer [Drugs for Alzheimer's disease: best avoided. No therapeutic advantage]. Prescrire International. June 2012;21(128):150.
PMID 22822592.
^ ab Querfurth HW, LaFerla FM (January 2010). "Alzheimer's disease". The New England Journal of Medicine. 362 (4): 329–44. doi:10.1056/NEJMra0909142. PMID 20107219.
^ ab GBD 2015 Disease Injury Incidence Prevalence Collaborators (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
^ ab GBD 2015 Mortality Causes of Death Collaborators (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–544. doi:10.1016/S0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
^ "About Alzheimer's Disease: Symptoms". National Institute on Aging. Archived from the original on 15 January 2012. Retrieved 28 December 2011.
^ Todd S, Barr S, Roberts M, Passmore AP (November 2013). "Survival in dementia and predictors of mortality: a review". International Journal of Geriatric Psychiatry. 28 (11): 1109–24. doi:10.1002/gps.3946. PMID 23526458.
^ "So, What Can You Do?". National Institute on Aging. 29 July 2016. Archived from the original on 3 April 2017.
^ abcde
Primary and secondary prevention trials in Alzheimer disease: looking back, moving forward. Current Alzheimer Research. 2017;14(4):426–40. doi:10.2174/1567205013666160930112125.
PMID 27697063.
^ abc Systematic Review of Information and Support Interventions for Caregivers of People with Dementia. BMC Geriatrics. 2007;7:18. doi:10.1186/1471-2318-7-18.
PMID 17662119.
^ Forbes D, Forbes SC, Blake CM, Thiessen EJ, Forbes S (April 2015). "Exercise programs for people with dementia". The Cochrane Database of Systematic Reviews (Submitted manuscript). 132 (4): 195–96. doi:10.1002/14651858.CD006489.pub4. PMID 25874613.
^ National Institute for Health and Clinical Excellence. "Low-dose antipsychotics in people with dementia". National Institute for Health and Care Excellence (NICE). Archived from the original on 5 December 2014. Retrieved 29 November 2014.
^ "Information for Healthcare Professionals: Conventional Antipsychotics". US Food and Drug Administration. 16 June 2008. Archived from the original on 29 November 2014. Retrieved 29 November 2014.
^ abc Evolution in the Conceptualization of Dementia and Alzheimer's Disease: Greco-Roman Period to the 1960s. Neurobiology of Aging. 1998;19(3):173–89. doi:10.1016/S0197-4580(98)00052-9.
PMID 9661992.
^ abcd Impact économique de la démence (English: The Economical Impact of Dementia). Presse Médicale. 2005;34(1):35–41. French. doi:10.1016/s0755-4982(05)83882-5.
PMID 15685097.
^ abcde Economic Considerations in Alzheimer's Disease. Pharmacotherapy. 1998;18(2 Pt 2):68–73; discussion 79–82. doi:10.1002/j.1875-9114.1998.tb03880.x.
PMID 9543467.
^ Evaluating Prescription Drugs Used to Treat: Alzheimer's Disease Comparing Effectiveness, Safety, and Price [PDF]. Consumer Reports Drug Effectiveness Review Project. May 2012. Consumer Reports.
^ abcde Recommendations for the Diagnosis and Management of Alzheimer's Disease and Other Disorders Associated with Dementia: EFNS Guideline. European Journal of Neurology. 2007;14(1):e1–26. doi:10.1111/j.1468-1331.2006.01605.x.
PMID 17222085.
^ abc Multiple Cognitive Deficits During the Transition to Alzheimer's Disease. Journal of Internal Medicine. 2004;256(3):195–204. doi:10.1111/j.1365-2796.2004.01386.x.
PMID 15324363.
^ Instrumental Activities of Daily Living: A Stepping-stone Towards Alzheimer's Disease Diagnosis in Subjects with Mild Cognitive Impairment?. Acta Neurologica Scandinavica. 2003;Suppl(179):42–46. doi:10.1034/j.1600-0404.107.s179.8.x.
PMID 12603250.
^ ab Neuropsychological Features of Mild Cognitive Impairment and Preclinical Alzheimer's Disease. Acta Neurologica Scandinavica. 2003;179:34–41. doi:10.1034/j.1600-0404.107.s179.7.x.
PMID 12603249.
^ Apathy in Alzheimer's Disease. Journal of the American Geriatrics Society. 2001;49(12):1700–07. doi:10.1046/j.1532-5415.2001.49282.x.
PMID 11844006.
^ Murray ED, Buttner N, Price BH (2012). "Depression and Psychosis in Neurological Practice". In Bradley WG, Daroff RB, Fenichel GM, Jankovic J. Bradley's neurology in clinical practice (6th ed.). Philadelphia, PA: Elsevier/Saunders. ISBN 978-1-4377-0434-1.
^ Grundman M, Petersen RC, Ferris SH, Thomas RG, Aisen PS, Bennett DA, Foster NL, Jack CR, Galasko DR, Doody R, Kaye J, Sano M, Mohs R, Gauthier S, Kim HT, Jin S, Schultz AN, Schafer K, Mulnard R, van Dyck CH, Mintzer J, Zamrini EY, Cahn-Weiner D, Thal LJ (January 2004). "Mild cognitive impairment can be distinguished from Alzheimer disease and normal aging for clinical trials". Archives of Neurology. 61 (1): 59–66. doi:10.1001/archneur.61.1.59. PMID 14732621.
^ abcdefghijklmnopqrs Clinical Features of Alzheimer's Disease. European Archives of Psychiatry and Clinical Neuroscience. 1999;249(6):288–90. doi:10.1007/s004060050101.
PMID 10653284.
^ Memory Deficits in Alzheimer's Patients: A Comprehensive Review. Neuropsychology Review. 1992;3(2):119–69. doi:10.1007/BF01108841.
PMID 1300219.
^ Implicit Memory Performance of Patients with Alzheimer's Disease: A Brief Review. International Psychogeriatrics. 1995;7(3):385–92. doi:10.1017/S1041610295002134.
PMID 8821346.
^ ab Language Performance in Alzheimer's Disease and Mild Cognitive Impairment: a comparative review. Journal of Clinical and Experimental Neuropsychology. July 2008;30(5):501–56. doi:10.1080/13803390701550128.
PMID 18569251.
^ abc Effect of Alzheimer's Disease on Communication Function. Journal of the South Carolina Medical Association. 1994;90(9):417–23.
PMID 7967534.
^ Sundowning and Circadian Rhythms in Alzheimer's Disease. The American Journal of Psychiatry. 2001;158(5):704–11. doi:10.1176/appi.ajp.158.5.704.
PMID 11329390.
^ When Home Caregiving Ends: A Longitudinal Study of Outcomes for Caregivers of Relatives with Dementia. Journal of the American Geriatrics Society. 1995;43(1):10–16. doi:10.1111/j.1532-5415.1995.tb06235.x.
PMID 7806732.
^ "What We Know Today About Alzheimer's Disease". Alzheimer's Association. Archived from the original on 7 October 2011. Retrieved 1 October 2011.While scientists know Alzheimer's disease involves progressive brain cell failure, the reason cells fail isn't clear.
^ Reitz C, Mayeux R (April 2014). "Alzheimer disease: epidemiology, diagnostic criteria, risk factors and biomarkers". Biochemical Pharmacology. 88 (4): 640–51. doi:10.1016/j.bcp.2013.12.024. PMC 3992261. PMID 24398425.
^ Heritability of different forms of memory in the Late Onset Alzheimer's Disease Family Study.. Journal of Alzheimer's Disease. 2011;23(2):249–55. doi:10.3233/JAD-2010-101515.
PMID 20930268.
^ Role of genes and environments for explaining Alzheimer disease. Arch. Gen. Psychiatry. 2006;63(2):168–74. doi:10.1001/archpsyc.63.2.168.
PMID 16461860.[unreliable medical source?]
^ abc Alzheimer's Disease. Lancet. 2006;368(9533):387–403. doi:10.1016/S0140-6736(06)69113-7.
PMID 16876668.
^ ab Genome-wide association studies in Alzheimer disease. Archives of Neurology. 2008;65(3):329–34. doi:10.1001/archneur.65.3.329.
PMID 18332245.
^ Translating cell biology into therapeutic advances in Alzheimer's disease. Nature. 1999;399(6738 Suppl):A23–31. doi:10.1038/19866.
PMID 10392577.
^ Familial Alzheimer's disease-linked presenilin 1 variants elevate βA1-42/1-40 ratio in vitro and in vivo [PDF]. Neuron. 1996;17(5):1005–13. doi:10.1016/S0896-6273(00)80230-5.
PMID 8938131.
^ FAD mutants unable to increase neurotoxic Aβ 42 suggest that mutation effects on neurodegeneration may be independent of effects on Abeta. Journal of Neurochemistry. 2007;101(3):674–81. doi:10.1111/j.1471-4159.2006.04391.x.
PMID 17254019.[unreliable medical source?]
^ Apolipoprotein E: high-avidity binding to beta-amyloid and increased frequency of type 4 allele in late-onset familial Alzheimer disease. Proceedings of the National Academy of Sciences of the United States of America. 1993;90(5):1977–81. doi:10.1073/pnas.90.5.1977.
PMID 8446617.
^ ab Apolipoprotein E4: a causative factor and therapeutic target in neuropathology, including Alzheimer's disease. Proceedings of the National Academy of Sciences of the United States of America. 2006;103(15):5644–51. doi:10.1073/pnas.0600549103.
PMID 16567625.
^ Cholesterol, APOE genotype, and Alzheimer disease: an epidemiologic study of Nigerian Yoruba. Neurology. 2006;66(2):223–27. doi:10.1212/01.wnl.0000194507.39504.17.
PMID 16434658.
^ APOE ε4 is not associated with Alzheimer's disease in elderly Nigerians. Annals of Neurology. 2006;59(1):182–85. doi:10.1002/ana.20694.
PMID 16278853.
^ ab Lambert JC, Ibrahim-Verbaas CA, Harold D, Naj AC, Sims R, Bellenguez C, DeStafano AL, Bis JC, Beecham GW, Grenier-Boley B, Russo G, Thorton-Wells TA, Jones N, Smith AV, Chouraki V, Thomas C, Ikram MA, Zelenika D, Vardarajan BN, Kamatani Y, Lin CF, Gerrish A, Schmidt H, Kunkle B, Dunstan ML, Ruiz A, Bihoreau MT, Choi SH, Reitz C, Pasquier F, Cruchaga C, Craig D, Amin N, Berr C, Lopez OL, De Jager PL, Deramecourt V, Johnston JA, Evans D, Lovestone S, Letenneur L, Morón FJ, Rubinsztein DC, Eiriksdottir G, Sleegers K, Goate AM, Fiévet N, Huentelman MW, Gill M, Brown K, Kamboh MI, Keller L, Barberger-Gateau P, McGuiness B, Larson EB, Green R, Myers AJ, Dufouil C, Todd S, Wallon D, Love S, Rogaeva E, Gallacher J, St George-Hyslop P, Clarimon J, Lleo A, Bayer A, Tsuang DW, Yu L, Tsolaki M, Bossù P, Spalletta G, Proitsi P, Collinge J, Sorbi S, Sanchez-Garcia F, Fox NC, Hardy J, Deniz Naranjo MC, Bosco P, Clarke R, Brayne C, Galimberti D, Mancuso M, Matthews F, Moebus S, Mecocci P, Del Zompo M, Maier W, Hampel H, Pilotto A, Bullido M, Panza F, Caffarra P, Nacmias B, Gilbert JR, Mayhaus M, Lannefelt L, Hakonarson H, Pichler S, Carrasquillo MM, Ingelsson M, Beekly D, Alvarez V, Zou F, Valladares O, Younkin SG, Coto E, Hamilton-Nelson KL, Gu W, Razquin C, Pastor P, Mateo I, Owen MJ, Faber KM, Jonsson PV, Combarros O, O'Donovan MC, Cantwell LB, Soininen H, Blacker D, Mead S, Mosley TH, Bennett DA, Harris TB, Fratiglioni L, Holmes C, de Bruijn RF, Passmore P, Montine TJ, Bettens K, Rotter JI, Brice A, Morgan K, Foroud TM, Kukull WA, Hannequin D, Powell JF, Nalls MA, Ritchie K, Lunetta KL, Kauwe JS, Boerwinkle E, Riemenschneider M, Boada M, Hiltuenen M, Martin ER, Schmidt R, Rujescu D, Wang LS, Dartigues JF, Mayeux R, Tzourio C, Hofman A, Nöthen MM, Graff C, Psaty BM, Jones L, Haines JL, Holmans PA, Lathrop M, Pericak-Vance MA, Launer LJ, Farrer LA, van Duijn CM, Van Broeckhoven C, Moskvina V, Seshadri S, Williams J, Schellenberg GD, Amouyel P (December 2013). "Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer's disease". Nature Genetics. 45 (12): 1452–58. doi:10.1038/ng.2802. PMC 3896259. PMID 24162737.
^ Variant of TREM2 associated with the risk of Alzheimer's disease. The New England Journal of Medicine. 2012;368(2):107–16. doi:10.1056/NEJMoa1211103.
PMID 23150908.
^ TREM2 variants in Alzheimer's disease. The New England Journal of Medicine. 2012;368(2):117–27. doi:10.1056/NEJMoa1211851.
PMID 23150934.
^ Mukherjee, S; Mez, J; Trittschuh, EH; Saykin, AJ; Gibbons, LE; Fardo, DW; Wessels, M; Bauman, J; Moore, M; Choi, SE; Gross, AL; Rich, J; Louden, DKN; Sanders, RE; Grabowski, TJ; Bird, TD; McCurry, SM; Snitz, BE; Kamboh, MI; Lopez, OL; De Jager, PL; Bennett, DA; Keene, CD; Larson, EB; EPAD Study, Group.; Investigators from, ACT.; Investigators from, ROS.; Investigators from, MAP.; Investigators from, ADNI.; Investigators from the University of Pittsburgh, ADRC.; Crane, PK (4 December 2018). "Genetic data and cognitively defined late-onset Alzheimer's disease subgroups". Molecular psychiatry. doi:10.1038/s41380-018-0298-8. PMID 30514930.
^ The Cholinergic Hypothesis of Alzheimer's Disease: a Review of Progress. Journal of Neurology, Neurosurgery, and Psychiatry. 1999;66(2):137–47. doi:10.1136/jnnp.66.2.137.
PMID 10071091.
^ Martorana A, Esposito Z, Koch G (August 2010). "Beyond the cholinergic hypothesis: do current drugs work in Alzheimer's disease?". CNS Neuroscience & Therapeutics. 16 (4): 235–45. doi:10.1111/j.1755-5949.2010.00175.x. PMID 20560995.
^ Amyloid Deposition as the Central Event in the Aetiology of Alzheimer's Disease. Trends in Pharmacological Sciences. 1991;12(10):383–88. doi:10.1016/0165-6147(91)90609-V.
PMID 1763432.
^ ab Alzheimer's disease-do tauists and baptists finally shake hands?. Trends in Neurosciences. 2002;25(1):22–26. doi:10.1016/S0166-2236(00)02031-2.
PMID 11801334.
^ Alpha- and Beta-secretase Activity as a Function of Age and Beta-amyloid in Down Syndrome and Normal Brain. Neurobiology of Aging. 2007;28(10):1493–506. doi:10.1016/j.neurobiolaging.2006.06.023.
PMID 16904243.
^ Alzheimer Disease and Down Syndrome: Factors in Pathogenesis. Neurobiology of Aging. 2005;26(3):383–89. doi:10.1016/j.neurobiolaging.2004.08.005.
PMID 15639317.
^ Apolipoprotein E, Dementia, and Cortical Deposition of Beta-amyloid Protein. The New England Journal of Medicine. 1995;333(19):1242–47. doi:10.1056/NEJM199511093331902.
PMID 7566000.
^ Transgenic mice:
- Alzheimer-type Neuropathology in Transgenic Mice Overexpressing V717F Beta-amyloid Precursor Protein. Nature. 1995;373(6514):523–27. doi:10.1038/373523a0.
PMID 7845465. - Comparison of Neurodegenerative Pathology in Transgenic Mice Overexpressing V717F Beta-amyloid Precursor Protein and Alzheimer's Disease. The Journal of Neuroscience. 1996;16(18):5795–811.
PMID 8795633. - Correlative Memory Deficits, Abeta Elevation, and Amyloid Plaques in Transgenic Mice. Science. 1996;274(5284):99–102. doi:10.1126/science.274.5284.99.
PMID 8810256. - Spatial Learning, Exploration, Anxiety, and Motor Coordination in Female APP23 Transgenic Mice with the Swedish Mutation. Brain Research. 2002;956(1):36–44. doi:10.1016/S0006-8993(02)03476-5.
PMID 12426044.
- Alzheimer-type Neuropathology in Transgenic Mice Overexpressing V717F Beta-amyloid Precursor Protein. Nature. 1995;373(6514):523–27. doi:10.1038/373523a0.
^ Long-term Effects of Abeta42 Immunisation in Alzheimer's Disease: Follow-up of a Randomised, Placebo-controlled Phase I Trial. Lancet. 2008;372(9634):216–23. doi:10.1016/S0140-6736(08)61075-2.
PMID 18640458.
^ Aß Oligomer-Induced Aberrations in Synapse Composition, Shape, and Density Provide a Molecular Basis for Loss of Connectivity in Alzheimer's Disease. The Journal of Neuroscience. 2007;27(4):796–807. doi:10.1523/JNEUROSCI.3501-06.2007.
PMID 17251419.
^ Cellular Prion Protein Mediates Impairment of Synaptic Plasticity by Amyloid-β Oligomers. Nature. 2009;457(7233):1128–32. doi:10.1038/nature07761.
PMID 19242475.
^ ab APP Binds DR6 to Cause Axon Pruning and Neuron Death via Distinct Caspases. Nature. 19 February 2009;457(7232):981–89. doi:10.1038/nature07767.
PMID 19225519.
^ Feuerstein, Adam (14 February 2017). "Merck Alzheimer's Drug Study Halted Early for Futility". New York City, NY, USA: TheStreet, Inc. Archived from the original on 16 February 2017.Merck Alzheimer's Drug Study Halted Early for Futility Independent study monitors concluded that there was "virtually no chance of finding a positive clinical effect."
^ Tau Proteins and Neurofibrillary Degeneration. Brain Pathology. 1991;1(4):279–86. doi:10.1111/j.1750-3639.1991.tb00671.x.
PMID 1669718.
^ Tau Pathology in Alzheimer Disease and Other Tauopathies. Biochimica et Biophysica Acta. 2005;1739(2–3):198–210. doi:10.1016/j.bbadis.2004.09.008.
PMID 15615638.
^ The Role of Tau Phosphorylation and Cleavage in Neuronal Cell Death. Frontiers in Bioscience. 2007;12:733–56. doi:10.2741/2097.
PMID 17127334.
^ Deane R, Zlokovic BV (April 2007). "Role of the blood-brain barrier in the pathogenesis of Alzheimer's disease". Current Alzheimer Research. 4 (2): 191–7. doi:10.2174/156720507780362245. PMID 17430246.
^ Interactions of metals and Apolipoprotein E in Alzheimer's disease. Frontiers in Aging Neuroscience. 12 June 2014;6:121. doi:10.3389/fnagi.2014.00121.
PMID 24971061. "Although we still do not know if the metal ion dyshomeostasis present in AD is a cause or consequence of the disease, there is a growing body of evidence showing a direct correlation between metal ions and key AD-related key proteins."
^ Oxidative Stress Signaling in Alzheimer's Disease. Current Alzheimer Research. December 2008;5(6):525–32. doi:10.2174/156720508786898451.
PMID 19075578.
^ Plant Metal Chaperones: A Novel Perspective in Dementia Therapy. Amyloid. 2009;16(2):81–83. doi:10.1080/13506120902879392.
PMID 20536399.
^
"Aluminium and Alzheimer's disease". Facts about dementia. Alzheimer's Society. Archived from the original on 27 October 2005. Retrieved 14 October 2005.
^ Bondy SC (January 2016). "Low levels of aluminum can lead to behavioral and morphological changes associated with Alzheimer's disease and age-related neurodegeneration". Neurotoxicology (Submitted manuscript). 52: 222–29. doi:10.1016/j.neuro.2015.12.002. PMID 26687397.
^ Kandimalla R, Vallamkondu J, Corgiat EB, Gill KD (March 2016). "Understanding Aspects of Aluminum Exposure in Alzheimer's Disease Development". Brain Pathology. 26 (2): 139–54. doi:10.1111/bpa.12333. PMID 26494454.
^ Occupational Risk Factors in Alzheimer's Disease: A Review Assessing the Quality of Published Epidemiological Studies. Occupational and Environmental Medicine. 2007;64(11):723–32. doi:10.1136/oem.2006.028209.
PMID 17525096.
^ ab Lidsky TI (May 2014). "Is the Aluminum Hypothesis dead?". Journal of Occupational and Environmental Medicine. 56 (5 Suppl): S73–79. doi:10.1097/jom.0000000000000063. PMC 4131942. PMID 24806729.
^ Yegambaram M, Manivannan B, Beach TG, Halden RU (2015). "Role of environmental contaminants in the etiology of Alzheimer's disease: a review". Current Alzheimer Research. 12 (2): 116–46. doi:10.2174/1567205012666150204121719. PMC 4428475. PMID 25654508.
^ Cigarette smoking is a risk factor for Alzheimer's disease: An analysis controlling for tobacco industry affiliation. Journal of Alzheimer's Disease. 2010;19(2):465–80. doi:10.3233/JAD-2010-1240.
PMID 20110594.
^ Neuroinflammation – An Early Event in Both the History and Pathogenesis of Alzheimer's Disease. Neuro-Degenerative Diseases. 2010;7(1–3):38–41. doi:10.1159/000283480.
PMID 20160456.
^ Air Pollution, Oxidative Stress, and Alzheimer's Disease. Journal of Environmental and Public Health. 2012;2012:472751. doi:10.1155/2012/472751.
PMID 22523504.
^ Miklossy J (August 2011). "Alzheimer's disease – a neurospirochetosis. Analysis of the evidence following Koch's and Hill's criteria". Journal of Neuroinflammation. 8 (1): 90. doi:10.1186/1742-2094-8-90. PMC 3171359. PMID 21816039.
^ Pisa D, Alonso R, Rábano A, Rodal I, Carrasco L (October 2015). "Different Brain Regions are Infected with Fungi in Alzheimer's Disease". Scientific Reports. 5 (1): 15015. doi:10.1038/srep15015. PMC 4606562. PMID 26468932.
^ Bartzokis G (August 2011). "Alzheimer's disease as homeostatic responses to age-related myelin breakdown". Neurobiology of Aging. 32 (8): 1341–71. doi:10.1016/j.neurobiolaging.2009.08.007. PMC 3128664. PMID 19775776.
^ Cai Z, Xiao M (2016). "Oligodendrocytes and Alzheimer's disease". The International Journal of Neuroscience. 126 (2): 97–104. doi:10.3109/00207454.2015.1025778. PMID 26000818.
^ abc Reisberg B, Franssen EH, Hasan SM, Monteiro I, Boksay I, Souren LE, Kenowsky S, Auer SR, Elahi S, Kluger A (1999). "Retrogenesis: clinical, physiologic, and pathologic mechanisms in brain aging, Alzheimer's and other dementing processes". European Archives of Psychiatry and Clinical Neuroscience. 249 Suppl 3 (3): 28–36. doi:10.1007/pl00014170. PMID 10654097.
^ Alves GS, Oertel Knöchel V, Knöchel C, Carvalho AF, Pantel J, Engelhardt E, Laks J (2015). "Integrating retrogenesis theory to Alzheimer's disease pathology: insight from DTI-TBSS investigation of the white matter microstructural integrity". BioMed Research International. 2015: 1–11. doi:10.1155/2015/291658. PMC 4320890. PMID 25685779.
^ Brenner Carson, Verna (2015). Caregiving for Alzheimer's Disease. New York: Springer New York Academy of Sciences. pp. 1–9. ISBN 978-1-4939-2406-6.
^ Neuropathologic Changes in Alzheimer's Disease. The Journal of Clinical Psychiatry. 2003;64 Suppl 9:7–10.
PMID 12934968.
^ Where, when, and in what form does sporadic Alzheimer's disease begin?. Current Opinion in Neurology. December 2012;25(Pt 6):708–14. doi:10.1097/WCO.0b013e32835a3432.
PMID 23160422.
^ Automated MRI Measures Identify Individuals with Mild Cognitive Impairment and Alzheimer's Disease. Brain. August 2009;132(Pt 8):2048–57. doi:10.1093/brain/awp123.
PMID 19460794.
^ Moan R. MRI Software Accurately IDs Preclinical Alzheimer's Disease. Diagnostic Imaging. 20 July 2009 [archived 16 May 2016; Retrieved 7 January 2013].
^ ab The Importance of Neuritic Plaques and Tangles to the Development and Evolution of AD. Neurology. 2004;62(11):1984–89. doi:10.1212/01.WNL.0000129697.01779.0A.
PMID 15184601.
^ Regional Distribution of Neurofibrillary Tangles and Senile Plaques in the Cerebral Cortex of Elderly Patients: A Quantitative Evaluation of a One-year Autopsy Population from a Geriatric Hospital. Cerebral Cortex. 1994;4(2):138–50. doi:10.1093/cercor/4.2.138.
PMID 8038565.
^ Lewy Body Pathology in Alzheimer's Disease. Journal of Molecular Neuroscience. 2001;17(2):225–32. doi:10.1385/JMN:17:2:225.
PMID 11816795.
^ Role of Protein Aggregation in Mitochondrial Dysfunction and Neurodegeneration in Alzheimer's and Parkinson's Diseases. Neuromolecular Medicine. 2003;4(1–2):21–36. doi:10.1385/NMM:4:1-2:21.
PMID 14528050.
^ Synapse Formation and Function is Modulated by the Amyloid Precursor Protein. The Journal of Neuroscience. 2006;26(27):7212–21. doi:10.1523/JNEUROSCI.1450-06.2006.
PMID 16822978.
^ Roles of Amyloid Precursor Protein and its Fragments in Regulating Neural Activity, Plasticity and Memory. Progress in Neurobiology. 2003;70(1):1–32. doi:10.1016/S0301-0082(03)00089-3.
PMID 12927332.
^ Roles of Proteolysis and Lipid Rafts in the Processing of the Amyloid Precursor Protein and Prion Protein. Biochemical Society Transactions. 2005;33(Pt 2):335–38. doi:10.1042/BST0330335.
PMID 15787600.
^ Amyloid Fibrils from the Viewpoint of Protein Folding. Cellular and Molecular Life Sciences. 2004;61(5):511–24. doi:10.1007/s00018-003-3264-8.
PMID 15004691.
^ Tauopathies. Cellular and Molecular Life Sciences. 2007;64(17):2219–33. doi:10.1007/s00018-007-7220-x.
PMID 17604998.
^ Sun, Wenyan; Samimi, Hanie; Gamez, Maria; Zare, Habil; Frost, Bess (23 July 2018). "Pathogenic tau-induced piRNA depletion promotes neuronal death through transposable element dysregulation in neurodegenerative tauopathies". Nature Neuroscience. 21 (8): 1038–48. doi:10.1038/s41593-018-0194-1. PMC 6095477. PMID 30038280.
^ Current Insights into Molecular Mechanisms of Alzheimer Disease and Their Implications for Therapeutic Approaches. Neuro-Degenerative Diseases. 2007;4(5):349–65. doi:10.1159/000105156.
PMID 17622778.
^ Alzheimer Mechanisms and Therapeutic strategies. Cell. 2012;148(6):1204–22. doi:10.1016/j.cell.2012.02.040.
PMID 22424230.
^ Neurotrophic and Neurotoxic Effects of Amyloid Beta Protein: Reversal by Tachykinin Neuropeptides. Science. 1990;250(4978):279–82. doi:10.1126/science.2218531.
PMID 2218531.
^ Mitochondrial Abeta: A Potential Cause of Metabolic Dysfunction in Alzheimer's Disease. IUBMB Life. 2006;58(12):686–94. doi:10.1080/15216540601047767.
PMID 17424907.
^ New Therapeutic Strategies and Drug Candidates for Neurodegenerative Diseases: p53 and TNF-alpha Inhibitors, and GLP-1 Receptor Agonists. Annals of the New York Academy of Sciences. 2004;1035:290–315. doi:10.1196/annals.1332.018.
PMID 15681814.
^ Heneka MT, Carson MJ, El Khoury J, Landreth GE, Brosseron F, Feinstein DL, Jacobs AH, Wyss-Coray T, Vitorica J, Ransohoff RM, Herrup K, Frautschy SA, Finsen B, Brown GC, Verkhratsky A, Yamanaka K, Koistinaho J, Latz E, Halle A, Petzold GC, Town T, Morgan D, Shinohara ML, Perry VH, Holmes C, Bazan NG, Brooks DJ, Hunot S, Joseph B, Deigendesch N, Garaschuk O, Boddeke E, Dinarello CA, Breitner JC, Cole GM, Golenbock DT, Kummer MP (April 2015). "Neuroinflammation in Alzheimer's disease". The Lancet. Neurology. 14 (4): 388–405. doi:10.1016/S1474-4422(15)70016-5. PMC 5909703. PMID 25792098.
^ New insights into brain BDNF function in normal aging and Alzheimer disease. Brain Research Reviews. 2008;59(1):201–20. doi:10.1016/j.brainresrev.2008.07.007.
PMID 18708092.
^ Neurotrophic factors in Alzheimer's disease: role of axonal transport. Genes, Brain, and Behavior. 2008;7(Suppl 1):43–56. doi:10.1111/j.1601-183X.2007.00378.x.
PMID 18184369.
^ The Accurate Diagnosis of Early-onset Dementia. International Journal of Psychiatry in Medicine. 2006;36(4):401–12. doi:10.2190/Q6J4-R143-P630-KW41.
PMID 17407994.
^ Therapeutic Approaches to Alzheimer's Disease. Brain. 2006;129(Pt 11):2840–55. doi:10.1093/brain/awl280.
PMID 17018549.
^ Dementia: Quick Reference Guide (PDF). London: (UK) National Institute for Health and Clinical Excellence. November 2006. ISBN 978-1-84629-312-2. Archived from the original (PDF) on 27 February 2008. Retrieved 22 February 2008.
^ Neural Correlates of Alzheimer's Disease and Mild Cognitive Impairment: A Systematic and Quantitative Meta-Analysis involving 1,351 Patients. NeuroImage. 2009;47(4):1196–206. doi:10.1016/j.neuroimage.2009.05.037.
PMID 19463961.
^ ab Clinical Diagnosis of Alzheimer's Disease: Report of the NINCDS-ADRDA Work Group under the Auspices of Department of Health and Human Services Task Force on Alzheimer's Disease. Neurology. 1984;34(7):939–44. doi:10.1212/wnl.34.7.939.
PMID 6610841.
^ ab Research Criteria for the Diagnosis of Alzheimer's Disease: Revising the NINCDS-ADRDA Criteria. Lancet Neurology. 2007;6(8):734–46. doi:10.1016/S1474-4422(07)70178-3.
PMID 17616482.
^ Reliability and validity of NINCDS-ADRDA criteria for Alzheimer's disease. The National Institute of Mental Health Genetics Initiative. Archives of Neurology. 1994;51(12):1198–204. doi:10.1001/archneur.1994.00540240042014.
PMID 7986174.
^ American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders: DSM-IV-TR (4th Edition Text Revision ed.). Washington, DC: American Psychiatric Association. ISBN 978-0-89042-025-6.
^ [Clinical aspects of dementia]. Hokkaido Igaku Zasshi. 1996;71(3):315–20. Japanese.
PMID 8752526.
^ The mini-mental state examination: a comprehensive review. Journal of the American Geriatrics Society. 1992;40(9):922–35. doi:10.1111/j.1532-5415.1992.tb01992.x.
PMID 1512391.
^ Early diagnosis of dementia: neuropsychology. Journal of Neurology. 1999;246(1):6–15. doi:10.1007/s004150050299.
PMID 9987708.
^ The Validation of a Caregiver Assessment of Dementia: the Dementia Severity Scale. Alzheimer Disease and Associated Disorders. 2005;19(4):186–94. doi:10.1097/01.wad.0000189034.43203.60.
PMID 16327345.
^ Awareness of Deficits and Anosognosia in Alzheimer's Disease. L'Encéphale. 2004;30(6):570–77. French. doi:10.1016/S0013-7006(04)95472-3.
PMID 15738860.
^ The Initial Symptoms of Alzheimer Disease: Caregiver Perception. Acta Médica Portuguesa. 2004;17(6):435–44. Portuguese.
PMID 16197855.
^ The Decreasing Prevalence of Reversible Dementias: An Updated Meta-analysis. Archives of Internal Medicine. 2003;163(18):2219–29. doi:10.1001/archinte.163.18.2219.
PMID 14557220.
^ Amyloid-Associated Depression: A Prodromal Depression of Alzheimer Disease?. Archives of General Psychiatry. 2008;65(5):542–50. doi:10.1001/archpsyc.65.5.542.
PMID 18458206. PMC 3042807.
^ Differential Diagnosis of Alzheimer's Disease. Neurology. 1997;48(5 Suppl 6):S2–9. doi:10.1212/WNL.48.5_Suppl_6.2S.
PMID 9153154.
^ Contribution of Depression to Cognitive Impairment and Dementia in Older adults. The Neurologist. 2007;13(3):105–17. doi:10.1097/01.nrl.0000252947.15389.a9.
PMID 17495754.
^ Zhang S, Smailagic N, Hyde C, Noel-Storr AH, Takwoingi Y, McShane R, Feng J (July 2014). "(11)C-PIB-PET for the early diagnosis of Alzheimer's disease dementia and other dementias in people with mild cognitive impairment (MCI)". The Cochrane Database of Systematic Reviews (7): CD010386. doi:10.1002/14651858.CD010386.pub2. PMID 25052054.
^ Smailagic N, Vacante M, Hyde C, Martin S, Ukoumunne O, Sachpekidis C (January 2015). "¹⁸F-FDG PET for the early diagnosis of Alzheimer's disease dementia and other dementias in people with mild cognitive impairment (MCI)". The Cochrane Database of Systematic Reviews. 1: CD010632. doi:10.1002/14651858.CD010632.pub2. PMID 25629415.
^ Diagnosis and Treatment of Dementia: 1. Risk Assessment and Primary Prevention of Alzheimer Disease. Canadian Medical Association Journal. 2008;178(5):548–56. doi:10.1503/cmaj.070796.
PMID 18299540.
^ Cardiovascular Risk Factors for Alzheimer's Disease. The American Journal of Geriatric Cardiology. 2007;16(3):143–49. doi:10.1111/j.1076-7460.2007.06696.x.
PMID 17483665.
^ Role of HMG-CoA Reductase Inhibitors in Neurological Disorders: Progress to Date. Drugs. 2007;67(15):2111–20. doi:10.2165/00003495-200767150-00001.
PMID 17927279.
^ Statins and Dementia. Current Atherosclerosis Reports. 2007;9(2):154–61. doi:10.1007/s11883-007-0012-9.
PMID 17877925.
^ McGuinness B, Craig D, Bullock R, Malouf R, Passmore P (July 2014). "Statins for the treatment of dementia". The Cochrane Database of Systematic Reviews. 7 (7): CD007514. doi:10.1002/14651858.CD007514.pub3. PMID 25004278.
^ NSAIDs for the Chemoprevention of Alzheimer's Disease. Sub-Cellular Biochemistry. 2007;42:229–48. doi:10.1007/1-4020-5688-5_11.
PMID 17612054.
^ Hoozemans JJ, Veerhuis R, Rozemuller JM, Eikelenboom P (February 2011). "Soothing the inflamed brain: effect of non-steroidal anti-inflammatory drugs on Alzheimer's disease pathology". CNS & Neurological Disorders Drug Targets. 10 (1): 57–67. doi:10.2174/187152711794488665. PMID 21143138.
^ Long term hormone therapy for perimenopausal and postmenopausal women. The Cochrane Database of Systematic Reviews. 2017;1:CD004143. doi:10.1002/14651858.CD004143.pub5.
PMID 28093732.
^ ab Cognitive reserve and Alzheimer disease. Alzheimer Disease and Associated Disorders. July 2006;20(2):112–17. doi:10.1097/01.wad.0000213815.20177.19.
PMID 16917199.
^ ab Systematic Review of the Effect of Education on Survival in Alzheimer's Disease. International Psychogeriatrics. 2009;21(1):25–32. doi:10.1017/S1041610208008053.
PMID 19026089.
^ Neergaard, Lauran (19 February 2011). "Speaking 2 Languages May Delay Getting Alzheimer's". The Denver Post. Associated Press. Archived from the original on 2 May 2014.
^ Cheng ST (September 2016). "Cognitive Reserve and the Prevention of Dementia: the Role of Physical and Cognitive Activities". Current Psychiatry Reports. 18 (9): 85. doi:10.1007/s11920-016-0721-2. PMC 4969323. PMID 27481112.
^ Farina N, Rusted J, Tabet N (January 2014). "The effect of exercise interventions on cognitive outcome in Alzheimer's disease: a systematic review". International Psychogeriatrics. 26 (1): 9–18. doi:10.1017/S1041610213001385. PMID 23962667.
^ abc Nutrition and the Risk of Alzheimer's Disease. BioMed Research International. 2013;2013. doi:10.1155/2013/524820.
PMID 23865055.
^ Diet and Alzheimer's disease risk factors or prevention: the current evidence. Expert Review of Neurotherapeutics. May 2011;11(5):677–708. doi:10.1586/ern.11.56.
PMID 21539488.
^ Western diet consumption and cognitive impairment: links to hippocampal dysfunction and obesity. Physiology & Behavior. 18 April 2011;103(1):59–68. doi:10.1016/j.physbeh.2010.12.003.
PMID 21167850.
^ Lifestyle-related Factors in Predementia and Dementia Syndromes. Expert Review of Neurotherapeutics. 2008;8(1):133–58. doi:10.1586/14737175.8.1.133.
PMID 18088206.
^ Caffeine intake and dementia: systematic review and meta-analysis. Journal of Alzheimer's Disease. 2010;20 Suppl 1:S187–204. doi:10.3233/JAD-2010-091387.
PMID 20182026.
^ The neuroprotective effects of cocoa flavanol and its influence on cognitive performance. British Journal of Clinical Pharmacology. July 2012;75(3):n/a–n/a. doi:10.1111/j.1365-2125.2012.04378.x.
PMID 22775434.
^ [Dietary flavonoids and human health]. Annales Pharmaceutiques Françaises. March 2011;69(2):78–90. doi:10.1016/j.pharma.2010.11.004.
PMID 21440100.
^ Vitamin A and Alzheimer's disease. Geriatrics & Gerontology International. April 2012;12(2):180–88. doi:10.1111/j.1447-0594.2011.00786.x.
PMID 22221326.
^ Retinoids for treatment of Alzheimer's disease. BioFactors. Mar–April 2012;38(2):84–89. doi:10.1002/biof.196.
PMID 22419567.
^ The possible role of antioxidant vitamin C in Alzheimer's disease treatment and prevention. American Journal of Alzheimer's Disease & Other Dementias. March 2013;28(2):120–25. doi:10.1177/1533317512473193.
PMID 23307795.
^ Vitamin C and Vitamin E for Alzheimer's Disease. The Annals of Pharmacotherapy. 2005;39(12):2073–80. doi:10.1345/aph.1E495.
PMID 16227450.
^ ab Farina, Nicolas; Llewellyn, David; Isaac, Mokhtar Gad El Kareem Nasr; Tabet, Naji (2017). "Vitamin E for Alzheimer's dementia and mild cognitive impairment". The Cochrane Database of Systematic Reviews. 4: CD002854. doi:10.1002/14651858.CD002854.pub5. ISSN 1469-493X. PMID 28418065.
^ Selenium and Alzheimer's disease: a systematic review. Journal of Alzheimer's Disease. 2011;26(1):81–104. doi:10.3233/JAD-2011-110414.
PMID 21593562.
^ Zinc diet and Alzheimer's disease: a systematic review. Nutritional Neuroscience. 1 September 2012;15(5):2–12. doi:10.1179/1476830512Y.0000000010.
PMID 22583839.
^ Avan A, Hoogenraad TU (2015). "Zinc and Copper in Alzheimer's Disease". Journal of Alzheimer's Disease (Review). 46 (1): 89–92. doi:10.3233/JAD-150186. PMID 25835420.
^ Folic Acid with or without Vitamin B12 for the Prevention and Treatment of Healthy Elderly and Demented people. The Cochrane Database of Systematic Reviews. 2008;(4):CD004514. doi:10.1002/14651858.CD004514.pub2.
PMID 18843658.
^ Effect of Folic Acid, with or without other B vitamins, on Cognitive Decline: Meta-analysis of Randomized trials. The American Journal of Medicine. June 2010;123(6):522–27.e2. doi:10.1016/j.amjmed.2010.01.017.
PMID 20569758.
^ Docosahexaenoic acid homeostasis, brain aging and Alzheimer's disease: Can we reconcile the evidence?. Prostaglandins, Leukotrienes, and Essential Fatty Acids. January 2013;88(1):61–70. doi:10.1016/j.plefa.2012.04.006.
PMID 22575581.
^ Burckhardt M, Herke M, Wustmann T, Watzke S, Langer G, Fink A (April 2016). "Omega-3 fatty acids for the treatment of dementia". The Cochrane Database of Systematic Reviews. 4: CD009002. doi:10.1002/14651858.CD009002.pub3. PMID 27063583.
^ Curcumin and Alzheimer's disease. CNS Neuroscience & Therapeutics. October 2010;16(5):285–97. doi:10.1111/j.1755-5949.2010.00147.x.
PMID 20406252.
^ Ginkgo Biloba for Cognitive Impairment and Dementia. The Cochrane Database of Systematic Reviews. 2009;(1):CD003120. doi:10.1002/14651858.CD003120.pub3.
PMID 19160216.
^ Cannabinoids for the treatment of dementia. The Cochrane Database of Systematic Reviews. 2009;(2):CD007204. doi:10.1002/14651858.CD007204.pub2.
PMID 19370677.
^ Bilkei-Gorzo A (December 2012). "The endocannabinoid system in normal and pathological brain ageing". Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences. 367 (1607): 3326–41. doi:10.1098/rstb.2011.0388. PMC 3481530. PMID 23108550.
^ abc Birks, Jacqueline S.; Harvey, Richard J. (2018). "Donepezil for dementia due to Alzheimer's disease". The Cochrane Database of Systematic Reviews. 6: CD001190. doi:10.1002/14651858.CD001190.pub3. ISSN 1469-493X. PMID 29923184.
^ ab Birks JS, Grimley Evans J (April 2015). "Rivastigmine for Alzheimer's disease". The Cochrane Database of Systematic Reviews (4): CD001191. doi:10.1002/14651858.CD001191.pub3. PMID 25858345.
^ Cholinesterases and the pathology of Alzheimer disease. Alzheimer Disease and Associated Disorders. 1995;9 Suppl 2:23–28. doi:10.1097/00002093-199501002-00005.
PMID 8534419.
^ The new cholinesterase inhibitors for Alzheimer's disease, part 2: illustrating their mechanisms of action. The Journal of Clinical Psychiatry. 2000;61(11):813–14. doi:10.4088/JCP.v61n1101.
PMID 11105732.
^ ab Cholinesterase inhibitors for Alzheimer's disease. The Cochrane Database of Systematic Reviews. 2006;(1):CD005593. doi:10.1002/14651858.CD005593.
PMID 16437532.
^ Cholinesterase inhibitors in mild cognitive impairment: a systematic review of randomised trials. PLoS Medicine. 2007;4(11):e338. doi:10.1371/journal.pmed.0040338.
PMID 18044984.
^ al.], edited by Brian K. Alldredge ... [et (2013). Applied therapeutics : the clinical use of drugs (10th ed.). Baltimore: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 2385. ISBN 978-1609137137.CS1 maint: Extra text: authors list (link)
^ ab Paradigm shift in neuroprotection by NMDA receptor blockade: memantine and beyond. Nature Reviews. Drug Discovery. 2006;5(2):160–70. doi:10.1038/nrd1958.
PMID 16424917.
^ "Memantine". US National Library of Medicine (Medline). 4 January 2004. Archived from the original on 22 February 2010. Retrieved 3 February 2010.
^ McShane R, Areosa Sastre A, Minakaran N (April 2006). "Memantine for dementia". The Cochrane Database of Systematic Reviews (2): CD003154. doi:10.1002/14651858.CD003154.pub5. PMID 16625572.
^ "Namenda prescribing information" (PDF). Forest Pharmaceuticals. Archived from the original (PDF) on 27 February 2008. Retrieved 19 February 2008. (primary source)
^ Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline. Annals of Internal Medicine. 2008;148(5):379–97. doi:10.7326/0003-4819-148-5-200803040-00009.
PMID 18316756.
^ The Effectiveness of Atypical Antipsychotics for the Treatment of Aggression and Psychosis in Alzheimer's Disease. The Cochrane Database of Systematic Reviews. 2006;(1):CD003476. doi:10.1002/14651858.CD003476.pub2.
PMID 16437455.
^ The Dementia Antipsychotic Withdrawal Trial (DART-AD): Long-term Follow-up of a Randomised Placebo-controlled Trial. Lancet Neurology. 9 January 2009;8(2):151–17. doi:10.1016/S1474-4422(08)70295-3.
PMID 19138567. Lay summary.
^ Declercq T, Petrovic M, Azermai M, Vander Stichele R, De Sutter AI, van Driel ML, Christiaens T (March 2013). "Withdrawal versus continuation of chronic antipsychotic drugs for behavioural and psychological symptoms in older people with dementia". The Cochrane Database of Systematic Reviews. 3 (3): CD007726. doi:10.1002/14651858.CD007726.pub2. hdl:1854/LU-3109108. PMID 23543555.
^ Huperzine A for Alzheimer's disease. The Cochrane Database of Systematic Reviews. 2008;(2):CD005592. doi:10.1002/14651858.CD005592.pub2.
PMID 18425924.
^ abcdefg American Psychiatric Association practice guideline for the treatment of patients with Alzheimer's disease and other dementias. The American Journal of Psychiatry. December 2007;164(12 Suppl):5–56.
PMID 18340692.
^ Cognitive rehabilitation combined with drug treatment in Alzheimer's disease patients: a pilot study. Clinical Rehabilitation. 2005;19(8):861–69. doi:10.1191/0269215505cr911oa.
PMID 16323385.
^ Practice parameter: management of dementia (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(9):1154–66. doi:10.1212/WNL.56.9.1154.
PMID 11342679.
^ Non-pharmacological interventions for wandering of people with dementia in the domestic setting. The Cochrane Database of Systematic Reviews. 2007;(1):CD005994. doi:10.1002/14651858.CD005994.pub2.
PMID 17253573.
^ Effectiveness and acceptability of non-pharmacological interventions to reduce wandering in dementia: a systematic review. International Journal of Geriatric Psychiatry. 2007;22(1):9–22. doi:10.1002/gps.1643.
PMID 17096455.
^ Abraha I, Rimland JM, Trotta FM, Dell'Aquila G, Cruz-Jentoft A, Petrovic M, Gudmundsson A, Soiza R, O'Mahony D, Guaita A, Cherubini A (16 March 2017). "Systematic review of systematic reviews of non-pharmacological interventions to treat behavioural disturbances in older patients with dementia. The SENATOR-OnTop series". BMJ Open. 7 (3): e012759. doi:10.1136/bmjopen-2016-012759. PMC 5372076. PMID 28302633.CS1 maint: Uses authors parameter (link)
^ Chung JC, Lai CK, Chung PM, French HP (2002). "Snoezelen for dementia". The Cochrane Database of Systematic Reviews (4): CD003152. doi:10.1002/14651858.CD003152. PMID 12519587.
^ Woods, B; O'Philbin, L; Farrell, EM; Spector, AE; Orrell, M (1 March 2018). "Reminiscence therapy for dementia". The Cochrane Database of Systematic Reviews. 3: CD001120. doi:10.1002/14651858.CD001120.pub3. PMID 29493789.
^ Effectiveness of simulated presence therapy for individuals with dementia: a systematic review and meta-analysis. Aging & Mental Health. November 2008;12(6):779–85. doi:10.1080/13607860802380631.
PMID 19023729.
^ Validation therapy for dementia. The Cochrane Database of Systematic Reviews. 2003;(3):CD001394. doi:10.1002/14651858.CD001394.
PMID 12917907.
^ Snoezelen for dementia. The Cochrane Database of Systematic Reviews. 2002;(4):CD003152. doi:10.1002/14651858.CD003152.
PMID 12519587. (up to date as of 2009)
^ Withdrawn: reality orientation for dementia. The Cochrane Database of Systematic Reviews. 2000;(3):CD001119. doi:10.1002/14651858.CD001119.pub2.
PMID 17636652.
^ Efficacy of an evidence-based cognitive stimulation therapy programme for people with dementia: randomised controlled trial. The British Journal of Psychiatry. 2003;183(3):248–54. doi:10.1192/bjp.183.3.248.
PMID 12948999.
^ Chang, Chun-Hung; Lane, Hsien-Yuan; Lin, Chieh-Hsin (2018). "Brain Stimulation in Alzheimer's Disease". Frontiers in Psychiatry. 9: 201. doi:10.3389/fpsyt.2018.00201. ISSN 1664-0640. PMC 5992378. PMID 29910746.
 This article incorporates text by Chun-Hung Chang, Hsien-Yuan Lane, and Chieh-Hsin Lin available under the CC BY 4.0 license.
This article incorporates text by Chun-Hung Chang, Hsien-Yuan Lane, and Chieh-Hsin Lin available under the CC BY 4.0 license.
^ A Randomized, Controlled Trial of a Home Environmental Intervention: Effect on Efficacy and Upset in Caregivers and on Daily Function of Persons with Dementia. The Gerontologist. 1 February 2001;41(1):4–14. doi:10.1093/geront/41.1.4.
PMID 11220813.
^ Maintenance of Effects of the Home Environmental Skill-building Program for Family Caregivers and Individuals with Alzheimer's Disease and Related Disorders. The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2005;60(3):368–74. doi:10.1093/gerona/60.3.368.
PMID 15860476.
^ "Treating Behavioral and Psychiatric Symptoms". Alzheimer's Association. 2006. Archived from the original on 25 September 2006. Retrieved 25 September 2006.
^ Visual Contrast Enhances Food and Liquid Intake in Advanced Alzheimer's Disease. Clinical Nutrition (Edinburgh, Scotland). 2004;23(4):533–38. doi:10.1016/j.clnu.2003.09.015.
PMID 15297089.
^ Dudek, Susan G. (2007). Nutrition Essentials for Nursing Practice. Hagerstown, Maryland: Lippincott Williams & Wilkins. p. 360. ISBN 978-0-7817-6651-7. Retrieved 19 August 2008.
^ Analysis of Patients' Rights: Dementia and PEG Insertion. British Journal of Nursing. 2006;15(1):18–20. doi:10.12968/bjon.2006.15.1.20303.
PMID 16415742.
^ Tube Feeding Patients with Dementia. Nutrition in Clinical Practice. 2006;21(2):142–46. doi:10.1177/0115426506021002142.
PMID 16556924.
^ Predictors of Mortality in Patients with Alzheimer's Disease Living in Nursing Homes. Journal of Neurology, Neurosurgery, and Psychiatry. 1999;67(1):59–65. doi:10.1136/jnnp.67.1.59.
PMID 10369823.
^ Medical issues:
- Palliative Care for Persons with Dementia. Home Healthcare Nurse. 2003;21(1):53–60; quiz 61. doi:10.1097/00004045-200301000-00012.
PMID 12544465. - Alzheimer's Disease: Psychopathology, Medical Management and Dental Implications. Journal of the American Dental Association. 2006;137(9):1240–51.
PMID 16946428. - Practical Guidelines for the Diagnosis and Management of Weight Loss in Alzheimer's Disease: A Consensus from Appropriateness Ratings of a Large Expert Panel. The Journal of Nutrition, Health & Aging. 2007;11(1):33–37.
PMID 17315078. - Training Caregivers to Change the Sleep Hygiene Practices of Patients with Dementia: The NITE-AD Project. Journal of the American Geriatrics Society. 2003;51(10):1455–60. doi:10.1046/j.1532-5415.2003.51466.x.
PMID 14511168. - Higher Respiratory Infection Rates on an Alzheimer's Special Care Unit and successful intervention. Journal of the American Geriatrics Society. 1995;43(12):1341–44. doi:10.1111/j.1532-5415.1995.tb06611.x.
PMID 7490383.
- Palliative Care for Persons with Dementia. Home Healthcare Nurse. 2003;21(1):53–60; quiz 61. doi:10.1097/00004045-200301000-00012.
^ Palliative Excellence in Alzheimer Care Efforts (PEACE): A Program Description. Journal of Palliative Medicine. 2003;6(2):315–20. doi:10.1089/109662103764978641.
PMID 12854952.
^ ab Zanetti O, Solerte SB, Cantoni F (2009). "Life expectancy in Alzheimer's disease (AD)". Archives of Gerontology and Geriatrics. 49 Suppl 1: 237–43. doi:10.1016/j.archger.2009.09.035. PMID 19836639.
^ ab Long-Term Survival and Predictors of Mortality in Alzheimer's Disease and Multi-Infarct Dementia. Acta Neurologica Scandinavica. 1995;91(3):159–64. doi:10.1111/j.1600-0404.1995.tb00426.x.
PMID 7793228.
^ Predictors of Mortality in Patients Diagnosed with Probable Alzheimer's Disease. Neurology. 1996;47(2):433–39. doi:10.1212/wnl.47.2.433.
PMID 8757016.
^ Survival after Initial Diagnosis of Alzheimer Disease. Annals of Internal Medicine. 2004;140(7):501–09. doi:10.7326/0003-4819-140-7-200404060-00008.
PMID 15068977.
^ Predictors of Survival with Alzheimer's Disease: A Community-based Study. Psychological Medicine. 1995;25(1):171–77. doi:10.1017/S0033291700028191.
PMID 7792352.
^ Functional Transitions and Active Life Expectancy Associated with Alzheimer Disease. Archives of Neurology. 2003;60(2):253–59. doi:10.1001/archneur.60.2.253.
PMID 12580712.
^ ab Alzheimer Disease and Mortality: A 15-year Epidemiological Study. Archives of Neurology. 2005;62(5):779–84. doi:10.1001/archneur.62.5.779.
PMID 15883266.
^ abc Incidence and subtypes of dementia in three elderly populations of central Spain. Journal of the Neurological Sciences. 2008;264(1–2):63–72. doi:10.1016/j.jns.2007.07.021.
PMID 17727890.
^ abc Incidence of dementia, Alzheimer's disease, and vascular dementia in Italy. The ILSA Study. Journal of the American Geriatrics Society. 2002;50(1):41–48. doi:10.1046/j.1532-5415.2002.50006.x.
PMID 12028245.
^ Gender Differences in the Incidence of AD and Vascular Dementia: The EURODEM Studies. EURODEM Incidence Research Group. Neurology. 1999;53(9):1992–97. doi:10.1212/wnl.53.9.1992.
PMID 10599770.
^ Tejada-Vera B. (2013). Mortality from Alzheimer's Disease in the United States: Data for 2000 and 2010. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics.
^ 2000 U.S. estimates:
- Alzheimer Disease in the US population: Prevalence Estimates Using the 2000 census. Archives of Neurology. 2003;60(8):1119–22. doi:10.1001/archneur.60.8.1119.
PMID 12925369.
"Profiles of General Demographic Characteristics, 2000 Census of Population and Housing, United States" (PDF). U.S. Census Bureau. 2001. Archived (PDF) from the original on 19 August 2008. Retrieved 27 August 2008.
- Alzheimer Disease in the US population: Prevalence Estimates Using the 2000 census. Archives of Neurology. 2003;60(8):1119–22. doi:10.1001/archneur.60.8.1119.
^ ab Global Prevalence of Dementia: A Delphi Consensus Study. Lancet. 2005;366(9503):2112–17. doi:10.1016/S0140-6736(05)67889-0.
PMID 16360788.
^ World Health Organization (2006). Neurological Disorders: Public Health Challenges. Switzerland: World Health Organization. pp. 204–07. ISBN 978-92-4-156336-9. Archived from the original on 10 February 2010.
^ 2006 prevalence estimate:
- Forecasting the global burden of Alzheimer's disease. Alzheimer's & Dementia. 2007;3(3):186–91. doi:10.1016/j.jalz.2007.04.381.
PMID 19595937. - World population prospects: the 2006 revision, highlights [PDF]. 2007.
- Forecasting the global burden of Alzheimer's disease. Alzheimer's & Dementia. 2007;3(3):186–91. doi:10.1016/j.jalz.2007.04.381.
^ Auguste D.:
- Alzheimer Alois. Über eine eigenartige Erkrankung der Hirnrinde [About a peculiar disease of the cerebral cortex]. Allgemeine Zeitschrift für Psychiatrie und Psychisch-Gerichtlich Medizin. 1907;64(1–2):146–48. (in German).
- About a Peculiar Disease of the Cerebral Cortex. Alzheimer Disease and Associated Disorders. 1987;1(1):3–8.
PMID 3331112.
Maurer Ulrike; Maurer Konrad (2003). Alzheimer: The Life of a Physician and the Career of a Disease. New York: Columbia University Press. p. 270. ISBN 978-0-231-11896-5.
^ Berrios G E. Alzheimer's Disease: A Conceptual History. Int. J. Ger. Psychiatry. 1990;5(6):355–65. doi:10.1002/gps.930050603.
^ Kraepelin Emil (17 January 2007). Clinical Psychiatry: A Textbook For Students And Physicians (Reprint). Translated by Diefendorf A. Ross. Kessinger Publishing. p. 568. ISBN 978-1-4325-0833-3.
^ Katzman Robert; Terry Robert D; Bick Katherine L, eds. (1978). Alzheimer's Disease: Senile Dementia and Related Disorders. New York: Raven Press. p. 595. ISBN 978-0-89004-225-0.
^ History of Dementia and Dementia in History: An Overview. Journal of the Neurological Sciences. 1998;158(2):125–33. doi:10.1016/S0022-510X(98)00128-2.
PMID 9702682.
^ Origin of the Distinction between Alzheimer's Disease and Senile Dementia: How History Can Clarify Nosology. Neurology. 1986;36(11):1497–99. doi:10.1212/wnl.36.11.1497.
PMID 3531918.
^ Economic Impact of Dementia in Developing Countries: An Evaluation of Costs of Alzheimer-type Dementia in Argentina. International Psychogeriatrics. 2007;19(4):705–18. doi:10.1017/S1041610206003784.
PMID 16870037.
^ The Economic Costs of Dementia in Korea, 2002. International Journal of Geriatric Psychiatry. 2006;21(8):722–28. doi:10.1002/gps.1552.
PMID 16858741.
^ An Estimate of the Worldwide Prevalence and Direct Costs of Dementia in 2003. Dementia and Geriatric Cognitive Disorders. 2006;21(3):175–81. doi:10.1159/000090733.
PMID 16401889.
^ abc Informal Costs of Dementia Care: Estimates from the National Longitudinal Caregiver Study. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences. 2001;56(4):S219–28. doi:10.1093/geronb/56.4.S219.
PMID 11445614.
^ Determinants of Costs of Care for Patients with Alzheimer's Disease. International Journal of Geriatric Psychiatry. 2006;21(5):449–59. doi:10.1002/gps.1489.
PMID 16676288.
^ ab "The MetLife study of Alzheimer's disease: The caregiving experience" (PDF). MetLife Mature Market Institute. August 2006. Archived from the original (PDF) on 8 January 2011. Retrieved 5 February 2011.
^ EUROCARE: a cross-national study of co-resident spouse carers for people with Alzheimer's disease: I—Factors associated with carer burden. International Journal of Geriatric Psychiatry. 1999;14(8):651–61. doi:10.1002/(SICI)1099-1166(199908)14:8<651::AID-GPS992>3.0.CO;2-B.
PMID 10489656.
^ EUROCARE: A Cross-National Study of Co-resident Spouse Carers for People with Alzheimer's Disease: II—A Qualitative Analysis of the Experience of Caregiving. International Journal of Geriatric Psychiatry. 1999;14(8):662–67. doi:10.1002/(SICI)1099-1166(199908)14:8<662::AID-GPS993>3.0.CO;2-4.
PMID 10489657.
^ ab Economic Considerations in the Management of Alzheimer's Disease. Clinical Interventions in Aging. 2006;1(2):143–54. doi:10.2147/ciia.2006.1.2.143.
PMID 18044111.
^ Early Community-based Service Utilization and Its Effects on Institutionalization in Dementia Caregiving. The Gerontologist. 2005;45(2):177–85. doi:10.1093/geront/45.2.177.
PMID 15799982.
^ The Dementias. Lancet. 2002;360(9347):1759–66. doi:10.1016/S0140-6736(02)11667-9.
PMID 12480441.
^ Psychosocial Effects on Carers of Living with Persons with Dementia. The Australian and New Zealand Journal of Psychiatry. 1990;24(3):351–61. doi:10.3109/00048679009077702.
PMID 2241719.
^ Determinants of Carer Stress in Alzheimer's Disease. International Journal of Geriatric Psychiatry. 1998;13(4):248–56. doi:10.1002/(SICI)1099-1166(199804)13:4<248::AID-GPS770>3.0.CO;2-0.
PMID 9646153.
^ A Systematic Review of the Effectiveness of Psychosocial Interventions for Carers of People with Dementia. Aging & Mental Health. 2001;5(2):107–19. doi:10.1080/13607860120038302.
PMID 11511058.
^ Bayley John (2000). Iris: A Memoir of Iris Murdoch. London: Abacus. ISBN 978-0-349-11215-2. OCLC 41960006.
^ Sparks Nicholas (1996). The notebook. Thorndike, Maine: Thorndike Press. p. 268. ISBN 978-0-7862-0821-0.
^ "Thanmathra". Webindia123.com. Archived from the original on 6 November 2007. Retrieved 24 January 2008.
^ Ogiwara Hiroshi (2004). Ashita no Kioku (in Japanese). Tōkyō: Kōbunsha. ISBN 978-4-334-92446-1. OCLC 57352130.
^ Munro Alice (2001). Hateship, Friendship, Courtship, Loveship, Marriage: Stories. New York: A.A. Knopf. ISBN 978-0-375-41300-1. OCLC 46929223.
^ "Malcolm and Barbara: A love story". Dfgdocs. Archived from the original on 24 May 2008. Retrieved 24 January 2008.
^
"Malcolm and Barbara: A love story". BBC Cambridgeshire. Archived from the original on 10 November 2012. Retrieved 2 March 2008.
^ Plunkett J (7 August 2007). "Alzheimer's film-maker to face ITV lawyers". London: Guardian Media. Archived from the original on 15 January 2008. Retrieved 24 January 2008.
^ Cummings JL, Morstorf T, Zhong K (July 2014). "Alzheimer's disease drug-development pipeline: few candidates, frequent failures". Alzheimer's Research & Therapy. 6 (4): 37. doi:10.1186/alzrt269. PMC 4095696. PMID 25024750.
^ New Class of Inhibitors of Beta-amyloid Fibril Formation. Implications for the Mechanism of Pathogenesis in Alzheimer's Disease. The Journal of Biological Chemistry. 2002;277(45):42881–90. doi:10.1074/jbc.M206593200.
PMID 12167652.
^ Intravenous Immunoglobulins as a Treatment for Alzheimer's Disease: Rationale and Current Evidence. Drugs. 2010;70(5):513–28. doi:10.2165/11533070-000000000-00000.
PMID 20329802.
^ Vaccination:
- Immunotherapy as Treatment for Alzheimer's Disease. Expert Review of Neurotherapeutics. 2007;7(11):1535–48. doi:10.1586/14737175.7.11.1535.
PMID 17997702. - Clinical Immunologic Approaches for the Treatment of Alzheimer's Disease. Expert Opinion on Investigational Drugs. 2007;16(6):819–28. doi:10.1517/13543784.16.6.819.
PMID 17501694. - Vaccination Strategies for Alzheimer's Disease: A New Hope?. Drugs & Aging. 2007;24(2):107–19. doi:10.2165/00002512-200724020-00003.
PMID 17313199.
- Immunotherapy as Treatment for Alzheimer's Disease. Expert Review of Neurotherapeutics. 2007;7(11):1535–48. doi:10.1586/14737175.7.11.1535.
^ "Study Evaluating ACC-001 in Mild to Moderate Alzheimers Disease Subjects". Clinical Trial. US National Institutes of Health. 11 March 2008. Archived from the original on 30 July 2013. Retrieved 5 June 2008.
^ "Study Evaluating Safety, Tolerability, and Immunogenicity of ACC-001 in Subjects with Alzheimer's Disease". US National Institutes of Health. Archived from the original on 29 October 2008. Retrieved 5 June 2008.
^ "Alzheimer's Disease Vaccine Trial Suspended on Safety Concern". Medpage Today. 18 April 2008. Archived from the original on 23 April 2008. Retrieved 14 June 2008.
^ "Bapineuzumab in Patients with Mild to Moderate Alzheimer's Disease/ Apo_e4 Non-carriers" (Clinical Trial). US National Institutes of Health. 29 February 2008. Archived from the original on 22 March 2008. Retrieved 23 March 2008.
^ Sperling RA, Jack CR, Black SE, Frosch MP, Greenberg SM, Hyman BT, Scheltens P, Carrillo MC, Thies W, Bednar MM, Black RS, Brashear HR, Grundman M, Siemers ER, Feldman HH, Schindler RJ (July 2011). "Amyloid-related imaging abnormalities in amyloid-modifying therapeutic trials: recommendations from the Alzheimer's Association Research Roundtable Workgroup". Alzheimer's & Dementia. 7 (4): 367–85. doi:10.1016/j.jalz.2011.05.2351. PMC 3693547. PMID 21784348.
^ "Safety, Tolerability and Efficacy Study to Evaluate Subjects with Mild Cognitive Impairment" (Clinical Trial). US National Institutes of Health. 11 March 2008. Archived from the original on 22 October 2008. Retrieved 23 March 2008.
^ "Study Evaluating the Safety, Tolerability and Efficacy of PBT2 in Patients with Early Alzheimer's Disease" (Clinical Trial). US National Institutes of Health. 13 January 2008. Archived from the original on 31 August 2008. Retrieved 23 March 2008.
^ Etanercept research:
- Tobinick E. Tumour necrosis factor modulation for treatment of Alzheimer's disease: rationale and current evidence. CNS Drugs. September 2009;23(9):713–25. doi:10.2165/11310810-000000000-00000.
PMID 19689163. - TNF-alpha Modulation for Treatment of Alzheimer's Disease: A 6-Month Pilot Study. Medscape General Medicine. 2006;8(2):25.
PMID 16926764. - Perispinal etanercept: Potential as an Alzheimer Therapeutic. Journal of Neuroinflammation. 2008;5:3. doi:10.1186/1742-2094-5-3.
PMID 18186919. - Perispinal Etanercept for Treatment of Alzheimer's Disease. Current Alzheimer Research. 2007;4(5):550–52. doi:10.2174/156720507783018217.
PMID 18220520. - Targeting TNF: a therapeutic strategy for Alzheimer's disease. Drug Discovery Today. 4 July 2014. doi:10.1016/j.drudis.2014.06.029.
PMID 24998784.
- Tobinick E. Tumour necrosis factor modulation for treatment of Alzheimer's disease: rationale and current evidence. CNS Drugs. September 2009;23(9):713–25. doi:10.2165/11310810-000000000-00000.
^ Tau aggregation inhibitor (TAI) therapy with remberTM arrests disease progression in mild and moderate Alzheimer's disease over 50 weeks. Alzheimer's & Dementia. 2008;4(4):T167. doi:10.1016/j.jalz.2008.05.438.
^ Methylthioninium chloride (MTC) acts as a tau aggregation inhibitor (TAI) in a cellular model and reverses tau pathology in transgenic mouse models of Alzheimer's disease. Alzheimer's & Dementia. 2008;4(4):T120–T121. doi:10.1016/j.jalz.2008.05.259.
^ Effect of dimebon on cognition, activities of daily living, behaviour, and global function in patients with mild-to-moderate Alzheimer's disease: a randomised, double-blind, placebo-controlled study. Lancet. 2008;372(9634):207–15. doi:10.1016/S0140-6736(08)61074-0.
PMID 18640457.
^ The rise and fall of Dimebon. Drug News & Perspectives. October 2010;23(8):518–23. doi:10.1358/dnp.2010.23.8.1500435.
PMID 21031168.
^ "Pfizer And Medivation announce results from two phase 3 studies in Dimebon (latrepirdine*) Alzheimer's disease clinical development program (NASDAQ:MDVN)" (Press release). Archived from the original on 4 September 2012. Retrieved 16 November 2012.
^ Translatability scoring in drug development: eight case studies. Journal of Translational Medicine. 2012;10(10):39. doi:10.1186/1479-5876-10-39.
PMID 22397594.
^ Baddeley TC, McCaffrey J, Storey JM, Cheung JK, Melis V, Horsley D, Harrington CR, Wischik CM (January 2015). "Complex disposition of methylthioninium redox forms determines efficacy in tau aggregation inhibitor therapy for Alzheimer's disease". The Journal of Pharmacology and Experimental Therapeutics. 352 (1): 110–18. doi:10.1124/jpet.114.219352. PMID 25320049.
^ Tau-aggregation inhibitor therapy for Alzheimer's disease. Biochem Pharmacol. 15 April 2014;88(4):529–39. doi:10.1016/j.bcp.2013.12.008.
PMID 24361915.
^ Effect of Meditation on Cognitive Functions in Context of Aging and Neurodegenerative Diseases. Frontiers in Behavioral Neuroscience. 2014;8:17. doi:10.3389/fnbeh.2014.00017.
PMID 24478663.
^ Larouche E, Hudon C, Goulet S (January 2015). "Potential benefits of mindfulness-based interventions in mild cognitive impairment and Alzheimer's disease: an interdisciplinary perspective". Behavioural Brain Research. 276 (276): 199–212. doi:10.1016/j.bbr.2014.05.058. PMID 24893317.
^ Jaunmuktane Z, Mead S, Ellis M, Wadsworth JD, Nicoll AJ, Kenny J, Launchbury F, Linehan J, Richard-Loendt A, Walker AS, Rudge P, Collinge J, Brandner S (September 2015). "Evidence for human transmission of amyloid-β pathology and cerebral amyloid angiopathy". Nature. 525 (7568): 247–50. doi:10.1038/nature15369. PMID 26354483. Archived from the original on 11 September 2015.
^ Abbott, Alison (2015). "Autopsies reveal signs of Alzheimer's in growth-hormone patients". Nature. 525 (7568): 165–66. doi:10.1038/525165a. PMID 26354460. Archived from the original on 11 September 2015.
^ ab Herpes simplex virus tipo 1 como factor de riesgo asociado con la enfermedad de Alzheimer [Herpes Simplex Virus Type 1 as Risk Factor Associated to Alzheimer Disease]. Revista Médica De Chile. June 2011;139(6):779–86. Spanish. doi:10.4067/S0034-98872011000600013.
PMID 22051760.
^ Herpes Simplex Virus type 1 DNA Is Located within Alzheimer's Disease Amyloid Plaques. The Journal of Pathology. 2008;217(1):131–38. doi:10.1002/path.2449.
PMID 18973185.
^ Itzhaki RF (2014). "Herpes simplex virus type 1 and Alzheimer's disease: increasing evidence for a major role of the virus". Frontiers in Aging Neuroscience. 6: 202. doi:10.3389/fnagi.2014.00202. PMC 4128394. PMID 25157230.
^ Itzhaki RF, Lathe R, Balin BJ, Ball MJ, Bearer EL, Braak H, Bullido MJ, Carter C, Clerici M, Cosby SL, Del Tredici K, Field H, Fulop T, Grassi C, Griffin WS, Haas J, Hudson AP, Kamer AR, Kell DB, Licastro F, Letenneur L, Lövheim H, Mancuso R, Miklossy J, Otth C, Palamara AT, Perry G, Preston C, Pretorius E, Strandberg T, Tabet N, Taylor-Robinson SD, Whittum-Hudson JA (2016). "Microbes and Alzheimer's Disease". Journal of Alzheimer's Disease. 51 (4): 979–84. doi:10.3233/JAD-160152. PMC 5457904. PMID 26967229. Archived from the original on 10 November 2016.
^ Alonso R, Pisa D, Rábano A, Carrasco L (July 2014). "Alzheimer's disease and disseminated mycoses". European Journal of Clinical Microbiology & Infectious Diseases. 33 (7): 1125–32. doi:10.1007/s10096-013-2045-z. PMID 24452965.
^ ab Pisa D, Alonso R, Rábano A, Rodal I, Carrasco L (October 2015). "Different Brain Regions are Infected with Fungi in Alzheimer's Disease". Scientific Reports. 5: 15015. doi:10.1038/srep15015. PMC 4606562. PMID 26468932. Archived from the original on 25 October 2016.
^ "Fungus, the bogeyman". The Economist. 22 October 2015. Archived from the original on 8 August 2017.
^ Kumar DK, Choi SH, Washicosky KJ, Eimer WA, Tucker S, Ghofrani J, Lefkowitz A, McColl G, Goldstein LE, Tanzi RE, Moir RD (May 2016). "Amyloid-β peptide protects against microbial infection in mouse and worm models of Alzheimer's disease". Science Translational Medicine. 8 (340): 340ra72. doi:10.1126/scitranslmed.aaf1059. PMC 5505565. PMID 27225182.
^ Kolata, Gina (25 May 2016). "Could Alzheimer's Stem From Infections? It Makes Sense, Experts Say". The New York Times. The New York Times. Archived from the original on 4 February 2017.
^ "Alzheimer's culprit may fight other diseases". Science News. 16 June 2016. Archived from the original on 26 May 2016.
^ Systematic Review of the Diagnostic Accuracy of 99mTc-HMPAO-SPECT in Dementia. The American Journal of Geriatric Psychiatry. 2004;12(6):554–70. doi:10.1176/appi.ajgp.12.6.554.
PMID 15545324.
^ The use of the exploratory IND in the evaluation and development of18F-PET radiopharmaceuticals for amyloid imaging in the brain: a review of one company's experience. The Quarterly Journal of Nuclear Medicine and Molecular Imaging. August 2009;53(4):387–93.
PMID 19834448.
^ Leung K (8 April 2010). "(E)-4-(2-(6-(2-(2-(2-(18F-fluoroethoxy)ethoxy)ethoxy)pyridin-3-yl)vinyl)-N-methyl benzenamine [[18F]AV-45]". Molecular Imaging and Contrast Agent Database. Archived from the original on 7 June 2010. Retrieved 24 June 2010.
^ Amyloid Imaging in Aging and Dementia: Testing the Amyloid Hypotheses in Vivo. Behavioural Neurology. 2009;21(1):117–28. doi:10.3233/BEN-2009-0232.
PMID 19847050. PMC 2804478.
^ Role of imaging techniques in the diagnosis of dementia. The British Journal of Radiology. December 2007;80(Spec No 2):S71–77. doi:10.1259/bjr/33117326.
PMID 18445747.
^ FDA recommends approval of new compound in Alzheimer's detection. JAMA. 19 January 2011;305(3):275–83. doi:10.1001/jama.2010.2008.
PMID 21245183.
^ "Amyvid". Community register of medicinal products for human use. European Community. 17 January 2013. Retrieved 18 April 2018.
^ Preclinical Alzheimer's disease: diagnosis and prediction of progression. Lancet Neurology. 1 September 2005;4(9):576–79. doi:10.1016/s1474-4422(05)70168-x.
PMID 16109364.
^ ab Sharma N, Singh AN (July 2016). "Exploring biomarkers for Alzheimer's disease". J Clin Diagn Res (Review). 10 (7): KE01–6. doi:10.7860/JCDR/2016/18828.8166. PMC 5020308. PMID 27630867.
Further reading
Listen to this article (info/dl)
Library resources about Alzheimer's Disease |
|
Alzheimer's Disease: Unraveling the Mystery. US Department of Health and Human Services, National Institute on Aging, NIH. 2008. Archived from the original on 8 January 2012.
Can Alzheimer's Disease Be Prevented? (PDF). US Department of Health and Human Services, National Institute on Aging, NIH. 2009. Archived from the original (PDF) on 2 May 2013.
Caring for a Person with Alzheimer's Disease: Your Easy-to-Use Guide from the National Institute on Aging. US Department of Health and Human Services, National Institute on Aging, NIH. 2009. Archived from the original on 8 January 2012.
Russell D, Barston S, White M (19 December 2007). "Alzheimer's Behavior Management: Learn to Manage Common Behavior Problems". helpguide.org. Archived from the original on 23 February 2008. Retrieved 29 February 2008.
- Greater cognitive deterioration in women than men with Alzheimer's disease: a meta analysis. Journal of Clinical and Experimental Neuropsychology. 2012;34(9):989–98. doi:10.1080/13803395.2012.712676.
PMID 22913619.
External links
| Wikimedia Commons has media related to Alzheimer's disease. |
| Classification | D
|
|---|---|
| External resources |
|
Alzheimer's disease at Curlie